

 13 June, 2016
13 June, 2016 




Informal healthcare providers are the most common, and sometimes the only source of healthcare, in much of rural India. In this post, Jishnu Das of the World Bank argues that informal providers should be trained and their impact evaluated to see if it improves healthcare for poor people.
Most of us would agree that when it comes to healthcare providers, some training is better than none. Yet even this seemingly innocuous statement is highly contentious in India, where training primary care providers who lack formal medical qualifications is anathema to the professional medical classes.
But the professionals are wrong. Training informal providers (IPs) could vastly improve the quality of care for millions of rural Indians and there is no evidence that it would make matters worse.
It is time to implement such training and critically evaluate its impact, to guide Indian states in deciding whether to treat these providers as an obstacle or an opportunity.
‘Teaching burglars how to steal’
But first, some background.
Most primary healthcare in India is private, accounting for more than 70% of total household spending and doctor visits (Raban et al. 2013, National Statistical Survey Organisation (NSSO), 2006). But the private sector has remained a bit of a mystery: the large household surveys on which such statistics are based do not ask who the private providers are. Recently, other surveys have revealed that, at least in rural areas, they are largely staffed by people with no formal medical qualifications and dubious legal standing.
In rural Madhya Pradesh for instance, 70% of healthcare providers working in the private sector lack any formal training — but they are the first point of contact for 77% of all doctor visits (Das et al. 2015). Similar numbers are found in states such as West Bengal, Rajasthan, Andhra Pradesh, and Uttarakhand. (Kanjilal et al. 2007, Gautham et al. 2013, Banerjee et al. 2004).
In essence, most of India’s medical care is provided by people who (legally) don’t exist.
These basic facts garner two kinds of reactions. One group believes that allowing IPs to practise amounts to dereliction of the state’s fundamental duty to provide healthcare. They argue that these providers should be arrested and that it is the public sector’s duty to increase the availability of qualified staff and guarantee quality of care.
According to this camp, all IPs are quacks, quackery is crookery and training quacks is “teaching burglars how to steal more effectively” (Pulla 2015a). As the chairman of the Andhra Pradesh Medical Council argued: “They are already violating rules. [After the training,] they will violate them even more” (Pulla 2015b).
There is a counterpoint though, which recognises that ramping up the size of public sector healthcare and improving governance to increase quality is a long slog. Meanwhile, training providers who have garnered the trust and respect of local people is valuable because it complements those long-term efforts.
Empirical vacuum
These two groups agree that IPs are uniquely responsible for many of the problems with the healthcare system, from misdiagnosis to antimicrobial resistance. However, Group 2 believes these problems can be alleviated through training. Group 1 believes that training will make the situation worse.
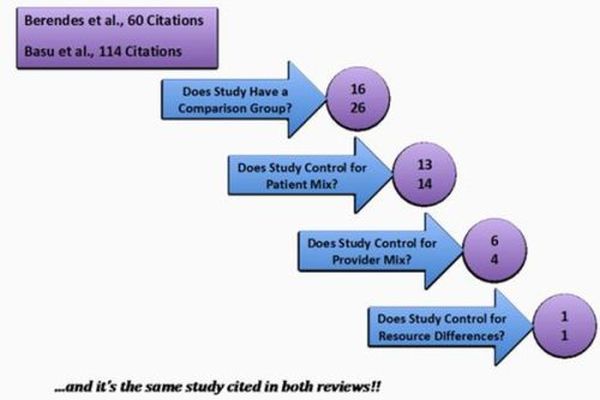
Much of this debate takes place in an empirical vacuum: when my colleagues and I tried to understand the reality on the ground, we could not find high-quality studies that conclusively evaluated the objective quality of care in the informal sector compared with formal clinics in the same area.
So, over five years, we worked with a multidisciplinary team to deploy ‘standardised patients’ among random samples of providers — both public sector and informal — in rural Madhya Pradesh (Das et al. 2012). These patients were recruited from local communities and trained to present the same condition to all providers exactly as a real patient would, both in terms of the biomedical symptoms and behaviour. This method is widely regarded as the ‘gold standard’ (Friedman 2013) when measuring healthcare quality.
Our research demonstrates two simple facts: that there are severe deficits in care quality across the board, and that IPs are the dominant source of care in rural India — the only source in some cases — because there isn’t a better, affordable option.
For example, only 5% of the villages in our sample had a fully qualified doctor, compared with an average of 1.8 IPs within each village and 3.6 just outside in the markets on the main roads.
Compared with interactions in the public sector, IPs spend more time with patients, and are more likely to adhere to checklists of medical history and national patient management guidelines. They are more likely to provide a diagnosis and are equally likely to correctly manage a case.
Unsurprisingly, fully qualified doctors in the private sector are more likely than IPs to correctly manage patients — but, worryingly, they are also more likely to use unnecessary antibiotics. And the highest rate of unnecessary antibiotic use, at 49%, was among the fully qualified providers in the public sector. So the perceived wisdom that widespread antibiotic resistance in India is driven by the irresponsible behaviour of IPs is incorrect.
Startling realities
This reality on the ground is more startling than even those who support IP training are willing to cede. Part of this reflects the abysmal training and practices of many supposedly qualified doctors in India. But part of it is also because IPs are seldom people who just closed the vegetable shop and opened a clinic. As we show in forthcoming research, 91% have received training, either by working in a clinic or as a pharmacist, or through some sort of observation in clinics and hospitals. This is a model of practical training, rather than formal medical education.
Whatever the reasons, the stark reality is that IPs are the backbone of India’s primary healthcare system. Our research clearly shows that their services are comparable with or better than alternatives in rural areas. Training can increase their knowledge base and, by extension, the quality of care available for millions of poor Indians.
I understand the anxiety around this: people are nervous about heading down an uncertain path that opens up a host of regulatory and conceptual problems. There is also the issue of challenging the authority of medical doctors, and the notion, enshrined in public health psyche, that qualifications are a proxy for quality.
And critical questions remain. What if training grants ‘official’ legitimacy to IPs, empowering them to give more antibiotics and try out dangerous procedures? And would training them take pressure off the state to provide decent public healthcare to poor people?
No one knows. We have never even tried to systematically evaluate the costs and benefits of training IPs. But given the evidence of their role, this is now a critical task.
This article previously appeared on SciDev.Net 2016 and the IGC Blog.
Further Reading
- Banerjee, Abhijeet , Angus Deaton and Esther Duflo (2004), ‘ Wealth, health, and health services in rural Rajasthan’, The American Economic Review, 92(2): 326-330.
- Das, J, A Holla, A Mohpal and K Muralidharan (2015) , ‘Quality and accountability in healthcare delivery: Audit evidence from primary care providers in India ,Policy Research Working Paper 7334, World Bank.
- Das, Jishnu, Alaka Holla, Veena Das, Manoj Mohanan, Diana Tabak and Brian Chan (2012), ‘In urban and rural India, a standardized patient study showed low levels of provider training and huge quality gaps’, Health Affairs, 31(12): 2774-2784.
- Friedman, J (2013) , ‘Feigning illness to improve care : Recent lessons from standardized patients in rural’ , Development Impact, World Bank, 16 January 2013.
- Gautham, Meenakshi, KM Shyamprasad, Rajesh Singh, Anshi Zachariah, Rajkumari Singh and Gerald Bloom (2014), ‘Informal rural healthcare providers in North and South India’ Health Policy and Planning, 29(1): 20-29.
- Kanjilal, B, S Mondal, T Samanta, A Mondal and S Singh (2007), ‘A Parallel Health Care market : Rural Medical Practitioners in West Bengal, India’, Research Brief, Future Heath Systems.
- NSSO (2006), ‘Morbidity, health care and the condition of the aged’, Central Statistics Office, Ministry of Statistics and Programme Implementation.
- Pulla, P (2015a), ‘India is training ‘quacks’ to do real medicine. This is why’, mosaic, 3 November 2015.
- Pulla, P (2015b) ‘Andhra Pradesh : the state that dared to train ‘quacks’ in medicine’ ,mosaic, 5 November 2015
- Raban, M, R Dondana, and L Dandona (2013), ‘Variations in catastrophic health expenditure estimates from household surveys in India’, Bulletin of the World Health Organization.

Comments will be held for moderation. Your contact information will not be made public.