

 27 April, 2023
27 April, 2023 






Agrawal et al. explore the role of gender-based preferences for demand of healthcare. Using CPHS data they find that the positive income shock – generated by a change in the mandated rates of contribution to the EPF – leads to a 11.6% decline in healthcare expenses driven by less expenditure on consultations and medications. However, this decline is not explained by women having better health outcomes and suggests that women, especially married women, prefer using the increased income on household goods.
Gender-based taste and preferences can significantly influence the allocation of monetary resources within a household (Banerjee et al. 2019). There is a rich literature on responses to cash transfers which analyses the role of additional income on allocation decisions of males and females. Many major existing anti-poverty transfer programmes in developing countries are targetted at women (Banerjee and Duflo 2019), based on the premise that women’s investment decisions and allocation of consumption expenditure appear to be more efficient (Goodman and Kaplan 2019). It is also widely acknowledged that responses to transfer payments will usually be distinct from shocks to earned income (Autor and Duggan 2007, Baird et al. 2011).
Transfer income seems to have a largely positive impact on healthcare. Increases in income result in increased use of healthcare services, more hospital visits, and the adoption of childcare facilities by the beneficiaries (Pitt et al. 2003, Gertler 2004, Morris et al. 2004, Rivera et al. 2004, Maluccio et al. 2005, Thornton 2008, Cahyadi et al. 2020). Although the willingness to spend on healthcare depends upon the access to quality services, opportunity cost of seeking treatment, the level of knowledge about the illness, and household income (Ensor and Cooper 2004, Gaarder et al. 2010, Chandra et al. 2011), we are interested in understanding whether specific ‘income shocks’ to women lead to changes in demand for healthcare as established in the cash transfer literature. Alternatively, it might be that women have different preferences than men when it comes to spending on healthcare – predominantly a credence good1 – when using their additional disposable income (Dulleck et al. 2011, Gottschalk et al. 2020).
Against this backdrop, in a recent study (Agrawal et al. 2022) we examine the impacts of a direct increase in disposable incomes of women engaged in formal employment in India on healthcare demand. Specifically, we exploit plausibly exogenous variation generated by a change in the rules of employee provident fund (EPF) contributions which was introduced by the Government of India on 1 February, 2018. The contributions to EPF were slashed from 12% to 8% for women employed in the formal sector. This led to an increased take-home salary for these women, and consequently a higher disposable income for the household compared to before the change. We find that women on average spend lesser on healthcare in response to this increase in their disposable incomes. While at face value this appears to suggest that healthcare is not being perceived as a normal good by women owing to the negative income elasticity of demand, a closer analysis suggests that substitution between the various components of healthcare expenditure can explain the overall effects.
Study design: Using macro data
The institutional structure of the EPF reform, which defines the eligibility rules for benefitting from the changes in the mandated contribution rates, represents a useful quasi-experimental setting. We employ a difference-in-differences framework2 to identify causal effects and provide reduced form intent-to-treat (ITT)3 effects of the reform on outcomes of interest. The point estimates capture the effect of the reduction in the contribution to EPF on the beneficiary household’s decision to allocate income that comes from the increment in take-home pay. We use Consumer Pyramid Household Survey (CPHS) data to identify two groups: the beneficiary group that receives the treatment (households dominated by women employed largely in the formal sector) and the control group that does not receive the treatment (households dominated by women employed largely in the non-formal sector).
CPHS provides us with a large panel data which covers more than 160,000 households spread across 28 states and 514 districts. We extract the data on the monthly consumption expenditure of households across the Indian economy between January 2016 and February 2020. This data provides information on the monthly expenditure of households on healthcare, divided further into expenditure on medicines, doctor’s consultation fees, medical tests, hospitalisation fees, contribution to insurance premiums and health enhancement activities. To examine the income allocation decision of a household apart from healthcare, we look at the monthly expenditure on 15 other categories of goods and services including food, clothing, intoxicants, education etc.
Using the survey information, our study measures the change in monthly expenditure on healthcare and other goods and services by households that received an additional income post February 2018 compared to households that did not.
Impact of income shock on healthcare expenditure
Our findings reveal a 11.6% decline in total health expenditure of beneficiary households as compared to the non-beneficiaries upon the infliction of EPF cuts. In other words, we find a reduction in monthly expenditure on healthcare by households that receive an additional income, as compared to households that do not receive the income benefit. The coefficient estimates for both healthcare as a whole and various categories of health expenditure have been highlighted graphically in Figure 1.
Figure 1. Impact of additional income on health expenditure of households
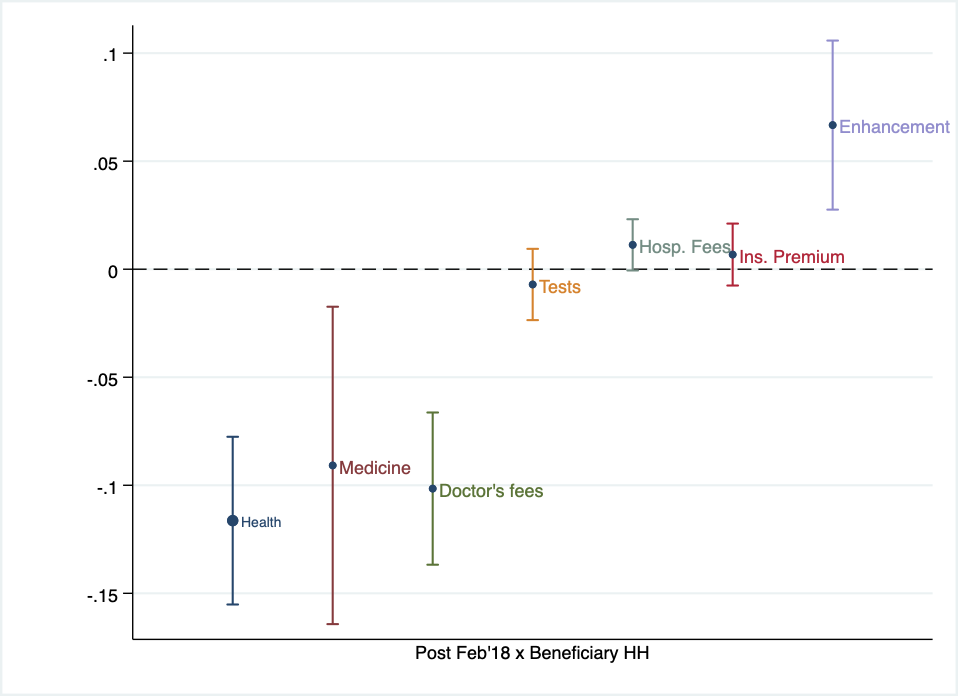
The decrease in total health expenditure is driven largely by a decrease in expenditure on medicine (9%) and expenses on doctor’s consultation (10%). This reduction in expenditure can partly be explained by improved health conditions of women, as they seem to be spending more on health enhancing activities such as gym subscriptions, hiring nutritionists etc. We find significant changes in the overall composition of household expenditure. Broadly, our findings suggest that female households that receive additional income do not prioritise health expenses when the income is not conditional to be spent upon a specific outcome.
Along with significant increases in human capital investments, we also see that beneficiary households allocate income towards purchasing clothes, footwear, jewellery and beauty products. We observe decreases in temptation consumption on goods such as recreation, intoxicants and restaurant dining. This vein of findings suggests that women have a different ‘taste’ for healthcare than men, and prefer to allocate increases in their own incomes to other components in the household production function.
Healthcare expenditure conditional to hospital visits
A potential channel for a decline in healthcare expenditure may be the reasoning that women, in general, have better health, which in turn leads to a decline in the need for health expenditure. To understand this channel further, we examine how women spend on healthcare after they decide to visit healthcare facilities (that is, when they have healthcare concerns). Our study captures the difference in the average expenditure of women employed in the formal sector (beneficiary) as compared to women employed in the non-formal sector (non-beneficiary) conditional on visiting the hospital and availing healthcare facilities, by employing a similar difference-in-differences framework.
For this purpose, we refer to the administrative electronic medical records of patients visiting the LV Prasad Eye Institute (LVPEI) between January 2016 and February 2020. LVPEI has a wide network of hospitals in the form of primary, secondary and tertiary centres across four states of India. Due to this pyramid structure, it witnesses an influx of patients for eye care from all socio-economic backgrounds. This widely representative dataset of a hospital system consists of 500,000 medical records, and provides information on the expenditure of an individual in a particular month at a centre for eye investigation and surgical treatment.
Interestingly, using the medical records data from hospital visits, we find a negative impact on healthcare spending (as indicated in Table 1). The coefficient in the top panel indicates that female beneficiaries visiting the eye hospital spend significantly less on surgical treatments as compared to female non-beneficiaries. This exercise essentially rules out the channel that better health explains the decline in health expenditure. Moreover, in the bottom panel, the coefficient estimate suggests that the marital status of a woman leads to a stronger negative impact on healthcare expenditure. These findings are in line with Mondal and Dubey (2020) who also find that there exists a large gender gap in hospital expenditure, especially in the case of currently married women. This suggests that married women might be contributing the additional income towards family welfare, which has also been echoed in past work (Doepke and Tertilt 2019). These findings provide evidence that women have different preferences when it comes to healthcare, and a positive income shock does not necessarily translate into increased healthcare spending.
Table 1. Impact of additional income on health expenditure for all female beneficiaries (top panel) and married women (bottom panel)
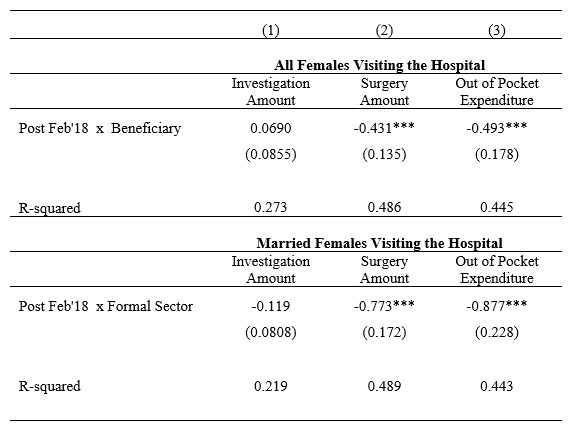
Notes: i) Our entire sample consists of 223,106 women, of which 168,491 are married women. ii) The dependent variables are log of the outcomes given in each column. iii) The estimation includes fixed effects for time, state of residence and center of the hospital along with a set of controls. iv) Standard errors (in parentheses below the coefficient) are clustered at district level, with ‘***’ indicating significance at 1%.
Insights
Our empirical examinations confirm the hypothesis that a positive change in income for women in developing countries, all else being equal, does not necessarily lead to an increase in healthcare spending, and in some cases may lead to a decline. Given that we are able to rule out that this is entirely due to better health outcomes, our findings indicate that healthcare might not be a normal good for women in these settings. In line with models from De Rock et al. (2022) and Hoddinott and Skoufias (2004) of inter-household decision-making, our study suggests that if women in developing countries have a strong preference towards contributing to the welfare of the household, a marginal increase in their income may not lead to an increase in individual consumption expenditure. Consequently, if women’s preferences in response to the income shock change in a way that healthcare expenditure is ranked lower and other consumption are ranked higher in the order of preference, it may be possible that an increase in income does not translate to an increase in healthcare demand. This type of skewed preference in favour of household goods can be due to social factors such as family or peer pressure in households in developing countries (Anukriti et al. 2020, Anukriti et al. 2022, Karim et al. 2022) or may just simply reflect a revealed preference among women consumers (Caplin and Dean 2011, Kline and Tartari 2016).
Notes:
- A credence good is a type of good whose quality cannot be observed by the consumer until after making the purchase, meaning it is difficult to assess its utility.
- Differences-in-differences is a technique used to compare the evolution of outcomes over time in similar groups, where one experienced an event – in this case, a positive income shock – which the other did not.
- ITT is used in case of imperfect compliance, where all those randomised into the control group do not get the treatment; while those randomised into the treatment group can choose not to take the treatment
Further Reading
- Agrawal, S, C Chatterjee and S Chatterjee (2022), 'Sweet Cash: Is Healthcare a Normal Good for Women in Developing Countries?', SSRN Research Paper.
- Anukriti, S, Catalina Herrera-Almanza, Praveen K Pathak and Mahesh Karra (2020), “Curse of the Mummy-ji: The Influence of Mothers-in-Law on Women in India”, American Journal of Agricultural Economics, 102(5): 1328-1351. Available here.
- Anukriti, S, Sungoh Kwon and Nishith Prakash (2022), “Saving for dowry: Evidence from rural India”, Journal of Development Economics, 154: 102750.
- Autor, David H and Mark G Duggan (2007), “Distinguishing income from substitution effects in disability insurance: Preliminary evidence from the Veteran’s Disability Compensation program”, American Economic Review, 97(2): 119-124.
- Baird, Sarah, Craig McIntosh, and Berk Ozler (2011), “Cash or Condition? Evidence from a Cash Transfer Experiment”, The Quarterly Journal of Economics, 126(4): 1709-1753.
- Banerjee, A, P Niehaus and T Suri (2019), ‘Universal basic income in the developing world’, NBER Working Paper 25598.
- Banerjee, AV and E Duflo (2019), Good Economics for Hard Times, Public Affairs, New York.
- Cahyadi, Nur, et al. (2020), “Cumulative Impacts of Conditional Cash Transfer Programs: Experimental Evidence from Indonesia”, American Economic Journal: Economic Policy, 12(4): 88-110.
- Caplin, Andrew and Mark Dean (2011), “Search, choice, and revealed preference”, Theoretical Economics, 6(1): 19-48.
- Chandra, Amitabh, David Cutler and Zirui Song (2011), “Who Ordered That? The Economics of Treatment Choices in Medical Care”, Handbook of Health Economics, 2: 397-432.
- De Rock, Bram, Tom Potoms and Denni Tommasi (2022), “Household Responses to Cash Transfers”, Economic Development and Cultural Change, 70(2): 625-652.
- Doepke, Matthias and Michele Tertilt (2019), “Does female empowerment promote economic development?”, Journal of Economic Growth, 24(4): 309-343.
- Dulleck, Uwe, Rudolf Kerschbamer and Matthias Sutter (2011), “The Economics of Credence Goods: An Experiment on the Role of Liability, Verifiability, Reputation, and Competition”, American Economic Review, 101(2): 526-55.
- Ensor, Tim and Stephanie Cooper (2004), “Overcoming barriers to health service access: Influencing the demand side”, Health Policy and Planning, 19(2): 69-79.
- Gaarder, Marie M, Amanda Glassman and Jessica E Todd (2010), “Conditional cash transfers and health: Unpacking the causal chain”, Journal of Development Effectiveness, 2(1), 6–50.
- Gertler, Paul (2004), “Do Conditional Cash Transfers Improve Child Health? Evidence from PROGRESA’s Control Randomized Experiment”, American Economic Review, 94(2): 336-341.
- Goodman, Rachael and Sarah Kaplan (2019), “Work-Life Balance as a Household Negotiation: A New Perspective from Rural India”, Academy of Management Discoveries, 5(4): 465-486.
- Gottschalk, Felix, Wanda Mimra and Christian Waibel (2020), “Health Services as Credence Goods: A Field Experiment”, The Economic Journal, 130(629): 1346-1383.
- Hoddinott, John and Emmanuel Skoufias (2004), “The impact of PROGRESA on food consumption”, Economic Development and Cultural Change, 53(1): 37-61.
- Karim, Shamsul, Caleb Kwong, Mili Shrivastava and Jagannadha Pawan Tamvada (2022), “My mother-in-law does not like it: Resources, social norms, and entrepreneurial intentions of women in an emerging economy”, Small Business Economics, 60: 409-431.
- Kline, Patrick and Melissa Tartari (2016), “Bounding the Labor Supply Responses to a Randomized Welfare Experiment: A Revealed Preference Approach”, American Economic Review, 106(4): 972-
- Maluccio, JA and R Flores, R (2005), ‘Impact evaluation of a conditional cash transfer program: The Nicaraguan Red de Protección Social’, Research Report, International Food Policy Research Institute.
- Mondal, Bidisha and Jay Dev Dubey (2020), “Gender discrimination in health-care expenditure: An analysis across the age-groups with special focus on the elderly”, Social Science & Medicine, 258:
- Morris, Saul S, Pedro Olinto, Rafael Flores, Eduardo AF Nilson and Ana C Figueiro´ (2004), “Conditional Cash Transfers Are Associated with a Small Reduction in the Rate of Weight Gain of Preschool Children in Northeast Brazil”, The Journal of Nutrition, 134(9): 2336-2341.
- Pitt, Mark M, Shahidur R Khandker, Omar Haider Chowdhury Daniel L Millimet (2003), “Credit programs for the poor and the health status of children in rural Bangladesh”, International Economic Review, 44(1): 87-118.
- Rivera, Juan A, Daniela Sotres-Alvarez, Jean-Pierre Habicht, Teresa Shamah and Salvador Villalpando (2004), “Impact of the Mexican Program for Education, Health, and Nutrition (Progresa) on Rates of Growth and Anemia in Infants and Young Children: A Randomized Effectiveness Study”, The Journal of the American Medical Association, 291(21): 2563-2570.
- Thornton, Rebecca L (2008), “The Demand for, and Impact of, Learning HIV status”, American Economic Review, 98(5): 1829-63.

By: Aditya Belose 21 December, 2023
This analysis is incredibly insightful, shedding light on the nuanced impact of income changes on healthcare spending among women in developing countries. Could these findings potentially influence policy approaches to improve healthcare access for women? I'd love to know more about the implications for healthcare policies in such contexts. Great work! Looking forward to more in-depth research like this.