

 21 January, 2021
21 January, 2021 






Urban slum-dwellers are among the groups that are most at-risk of Covid-19, and their precarious situation is further compounded by rampant misinformation regarding the Virus. Based on a survey of about 4,000 households in slum areas in Uttar Pradesh, this article shows that recorded phone messages from doctors giving information on Covid-19 – along with high financial incentives to pay attention – can debunk related fake news.
The Director-General of the World Health Organization (WHO), Tedros Adhanom Ghebreyesus, stated in March 2020 that “[W]e're not just fighting a pandemic; we're fighting an infodemic”, referring to fake news about Covid-19 and how to prevent the spread of misinformation. While fake news about the Virus has been a global phenomenon, India is among the countries that are particularly struggling with reliable sources of information frequently being drowned out by unverified ones on the internet. In a new study, we explore ways to debunk fake news in the slums of India and demonstrate that mobile technology can effectively be used for this purpose (Armand, Augsburg and Bancalari 2021).
Background
One of the groups most at-risk of Covid-19 is the urban poor, living in overcrowded conditions with very limited access to public (health) infrastructure. One billion people live in such settlements (slums hereafter) – more than half of these in Asia and almost a fifth in India (World Bank, 2020). Their ability to follow advice by government and scientists on mitigation strategies – such as handwashing and social distancing – has been significantly hampered by the hardships they face on a daily basis, which include lack of access to water and sanitation systems at home and overcrowded living conditions (Brown et al. 2020, Afridi et al. 2020). Social distancing is more an aspiration than an attainable reality for urban slum-dwellers (Wasdani and Prasad 2020). Further, most slum-dwellers are daily-wage workers, which makes them more vulnerable to losing their jobs in lockdown conditions (Corburn et al. 2020).
In addition to these hardships, misinformation about the ways to prevent Covid-19 is widespread. Examples of such misinformation include that you cannot get infected if you are vegetarian, that warm weather can kill the Virus, and that Indians are immune to it. Such misinformation about ways to prevent Covid-19 is rampant on social media.1
The cost of misinformation
Misinformation imposes private and social costs by making it more difficult to infer the true state of the pandemic. In the presence of widespread misinformation, slum residents are at risk of falling into a false sense of protection and engaging in risky behaviours. Furthermore, the pandemic has forced decision-making to take place under great uncertainty, which makes individuals systematically less risk averse (Callen et al. 2014). In the US, for instance, misinformation2 spread through television shows and this led to a delay in the adoption of preventive behaviour (Bursztyn et al. 2020).
The Government of India, as most other governments in the world, is looking to find effective means through which to communicate the right ways to prevent the spread of this lethal Virus. Studies exploring means to nudge behaviours that affect public health (Alatas et al. 2019), including specific to Covid-19 (Banerjee et al. 2020), find that communication technologies and social media can be effective and low-cost tools. However, evidence about their effectiveness to correct ingrained misconceptions remains limited.
Using mobile technology to debunk misinformation
We study how fake news about Covid-19 can be debunked by making use of mobile technology. We do so in the context of slums in the cities of Lucknow and Kanpur in the state of Uttar Pradesh. We rely on a census of more than 30,000 households located in 142 slums, collected in 2018. For this study, we interview approximately 4,000 randomly selected households from this population pre- and post-intervention.
In particular, we seek to assess the effectiveness of doctors’ messages in countering misinformation about the prevention of Covid-19. For this, we conduct an experiment in which we randomly allocate households to either receive a recorded message from a doctor working in a locally well-known hospital, debunking fake news about Covid-19 (‘treatment’), or a message debunking fake news of Bollywood (‘control'). Messages were sent via mobile phones and, for the treatment group, centred around the idea that ‘eating vegetarian food does not fully protect one from Covid-19’.
Because uptake of messages via mobile phones can be extremely low, the effectiveness of these tools can be limited. For instance, Banerjee et al. (2020) achieved a viewing rate of information videos of only 1.14%, consistent with low rates of other ‘click-through’ studies (Richardson et al. 2007, Kanich et al. 2009). To overcome this limitation, we further explore if financial rewards lead to a higher uptake of messages. We cross-randomised3 treatment (doctors’ messages about Covid-19) and control (unrelated messages) households to participate in a ‘high-incentive’ lottery where they could win Rs. 5,000, or a ‘low-incentive’ lottery, where the winning amount was Rs. 2,500, conditional on listening and paying attention to the message. We collect data in the follow-up surveys of whether participants recall receiving a message about Covid-19 via voice messages or WhatsApp.
Doctors’ messages debunking fake news about ways to prevent Covid-19 can counter misinformation
Receiving a doctors’ message increases the probability of disagreeing with fake news about Covid-19 – albeit only when incentivised with the high-lottery amount. However, this impact is found in the participants’ response to survey questions pertaining to fake news that was not directly addressed by the doctors. While the doctors discussed that ‘eating vegetarian food does not fully protect one from Covid-19’, we find that the intervention increases the probability of disagreeing with the statement “Indians have a stronger immune system against the Virus” among highly incentivised individuals by 30%, compared to the effect on low-incentivised individuals.
Receiving a doctor’s message along with a low incentive to listen/pay attention, ‘crowds out’ investment of time to get informed about how to prevent the Virus (13% less than the average for the low-incentive group who receive Bollywood messages), as well as the probability of sharing information or advice with someone else about Covid-19 (17% less than the average for the low-incentive groups who receive Bollywood messages). These effects are offset when providing high incentives to pay attention to the doctors’ messages.
Figure 1. Impact of high and low incentives on information dissemination
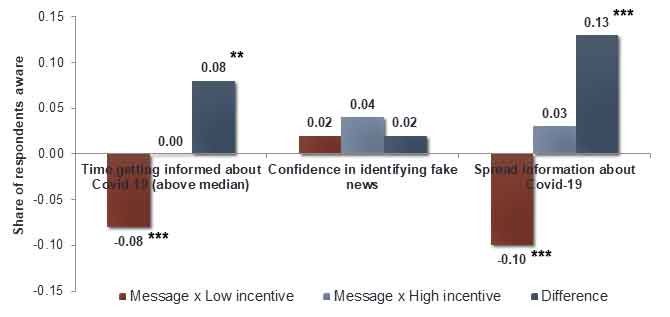
Notes: (i) Excluded group is the ‘control’ group that did not receive any message under the study. (ii) ‘Message’ indicates the group that received the intervention, that is, in which the household received the message from the doctor. (iii) ‘Low (high) incentive’ indicate the group in which the financial incentive is low (high). (iv) ‘Difference’ is the estimated difference between Message x Low incentive and Message x High incentive. (v)*** (**) denotes statistical significance at the 1(5)% level.4
Policy recommendations
Our study shows that doctors’ messages debunking fake news about ways to prevent Covid-19, accompanied by high incentives to listen/pay attention, can be a useful and cost-effective tool to counteract misinformation. It is, however, essential to find the optimal level of financial reward that triggers a positive behavioural response in different contexts, as a less-than-optimal level can crowd-out investment in time getting informed about prevention, and have the recipients disseminate this further. It is important to incentivise people to invest time in obtaining information about Covid-19 from trustworthy sources (reputable doctors, in our context).
In addition to debunking fake news, policymakers can consider using informational videos by doctor (with high incentives to watch/pay attention) in order to spread information about social distancing and vaccination.
I4I is now on Telegram. Please click here (@Ideas4India) to subscribe to our channel for quick updates on our content
Notes:
- The Government of India created a factsheet debunking the most common fake news.
- TV show downplaying the threat of Covid-19.
- Cross-randomisation is the allocation of half the subjects in the study to receive one arm of the intervention and the other half to receive the other arm of the intervention.
- With p < 0.01 (1% level), where the p-value is the probability of getting results at least as extreme as the results observed, given the assumption that the null hypothesis is true. A p-value lower than a mentioned significance level would be considered statistically significant (if p < 0.01(0.05), it is statistically significant at the 1%(5%) level)
Further Reading
- Afridi, F, A Dhillon and S Roy (2020), 'How has COVID-19 crisis affected the urban poor? Findings from a phone survey', Ideas for India, 23 April.
- Armand, A, B Augsburg and A Bancalari (2021), 'Coping with COVID-19 measures in informal settlements', IGC Working Paper.
- Banerjee, A, M Faye, A Kreuger, P Niehaus and T Suri (2020), 'Effects of a Universal Basic Income during the Pandemic', Working paper.
- Brown, C, M Ravallion and D van de Walle (2020), 'Can the World's Poor Protect Themselves from the New Coronavirus?', NBER Working Paper 27200.
- Bursztyn, L, A Rao, CP Roth and DH Yanagizawa-Drott (2020), 'Misinformation During A Pandemic', NBER Working Paper 27417.
- Callen, Michael, Mohammed Isaqzadeh, James D Long and Charles Sprenger (2014), "Violence and Risk Preference: Experimental Evidence from Afghanistan", American Economic Review, 104(1): 123-148.
- Corburn, Jason, David Vlahov, Blessing Mberu, Lee Riley, Waleska Teixeira Caiaffa, Sabina Faiz Rashid, Albert Ko, Sheela Patel, Smurti Jukur, Eliana Martínez-Herrera, Saroj Jayasinghe, Siddharth Agarwal, Blaise Nguendo-Yongsi, Jane Weru, Smith Ouma, Katia Edmundo, Tolu Oni and Hany Ayad (2020), "Slum Health: Arresting COVID-19 and Improving Well-Being in Urban Informal Settlements", Journal of Urban Health, 97(3): 348-357.
- Dupas, Pascaline (2014), "Short-Run Subsidies and Long-Run Adoption of New Health Products: Evidence from a Field Experiment", Econometrica, 82(1): 197-228.
- Kanich, Chris, Christian Kreibich, Kirill Levchenko, Brandon Enright, Geoffrey M Voelker, Vern Paxson and Stefan Savage (2009), "Spamalytics: an empirical analysis of spam marketing conversion", Communications of the ACM, 52(9): 99-107.
- Kirsch, P, H Kube and Zohlnhöfer (2020), 'Anti-corona-massnahmen: Grosse mehrheit hält sich an die vorgaben', 23 July, Working Paper.
- Lazarus, Jeffrey V, Scott C Ratzan, Adam Palayew, Lawrence O Gostin, Heidi J Larson, Kenneth Rabin, Spencer Kimball and Ayman El-Mohandes (2020), "A global survey of potential acceptance of a COVID-19 vaccine", Nature Medicine.
- Ministry of Home Affairs (2011), 'HH-8: Slum households by availability of type of latrine facility', Census of India.
- Richardson, M, E Dominowska and R Ragno (2007), 'Predicting Clicks: Estimating the Click-Through Rate for New Ads', Proceedings of the 16th International World Wide Web Conference (WWW-2007).
- Wasdani, Kishinchand Poornima and Ajnesh Prasad (2020), "The impossibility of social distancing among the urban poor: the case of an Indian slum in the times of COVID-19", Local Environment, 25(5): 414-418.
- World Bank (2020), World Development Indicators, DataBank (The World Bank).

Comments will be held for moderation. Your contact information will not be made public.