

 21 September, 2021
21 September, 2021 









Public health emergencies such as Covid-19 disproportionally cause mental health problems among women due to factors such as their inferior socioeconomic position in the household, greater care responsibilities, and risk of intimate partner violence. Based on a field study in rural Bangladesh, this article shows that a low-cost telecounselling intervention can effectively improve women’s mental health in resource-poor settings.
Women in developing countries, particularly those residing in rural regions, have limited access to mental health support owing to low levels of State capacity and resources.. With the onset of the Covid-19 pandemic, the psychological stress among these women has been on the rise due to the socioeconomic impact of the spread of the disease and the associated lockdowns that were implemented in order to arrest further transmission of the virus. To address the poor mental health conditions during the pandemic, we provided rural women in Bangladesh with a brief, light-touch, and low-cost telephone-based counselling (telecounselling) intervention (Vlassopoulos et al. 2021).
Mental health during the pandemic
Psychological distress has often been identified as one of the major consequences of environmental and natural disasters (Stain et al. 2011, Ho et al. 2014), health or financial crises (Lund et al. 2010, Mucci et al. 2016), and epidemics (Chua et al. 2004, Cowling et al. 2010, James et al. 2019). These effects can have a long-lasting effect on the both the mental and physical health of individuals. Since the onset of the Covid-19 pandemic, mental health experts have been expressing caution about the high incidence of stress and depression among people, due to the heavy socioeconomic burden of the pandemic and isolation (Holmes et al. 2020, Brooks et al. 2020; Galea et al. 2020). The consequences of the pandemic have been multidimensional and complex with over 4.5 million people losing their lives, and large number of survivors suffering from post-infection morbidities. The livlihoods of scores of people have been hit due to massive disruptions in economic activities, halt in production chains, and closure of markets. In the short run, preventive measures to check the spread of the disease have impacted the emotional and psychological health of residents of low and lower-middle income countries more harshly due to their fragile heathcare system, high population density, and limited resources and social safety nets.
The context
Bangladesh experienced a major economic setback during the pandemic due to a combination of factors, including interrupted domestic economic activities and reduced exports. Consequently, there has been a sharp decline in income, with millions losing their livelihood completely or partially (Ahmed et al. 2021). A large proportion of the population fell into poverty and became food insecure, which can potentially lead to mental health problems such as stress, anxiety, and depression. Prolonged isolation and persistent concern related to limited access to quality healthcare for one’s self and one’s family, which is a common scenario in the context of the Covid-19 pandemic, can amplify these feelings.
In Bangladesh, women are more likely to be disproportionally affected by mental health problems because of their disadvantageous socioeconomic position compared to men in the household, greater burden of daily chores, critical role in managing household food shortages, care responsibilities for children, elderly, and sick family members, and the risk of being victims of intimate partner violence (Ravindran and Shah 2020). Consequently, the mental well-being of women living in rural Bangladesh could deteriorate due to the lack of resources, and poor mental health support mechanisms (Rahman et al. 2021).
Our study
Our intervention (Vlassopoulos et al. 2021) included four brief modules, carefully developed and adapted to suit the purpose and the context, following Covid-19 mental health and psychosocial support guidelines prescribed by the International Federation of Red Cross (2020) and the World Health Organization (2020), and incorporating important components from mental health literature (Brooks et al. 2020). The four modules cover the following four major elements: (i) Behavioural: problem-solving, behavioural activation, relaxation, and exposure to information related to the Virus, safety precautions, etc.; (ii) Interpersonal: identifying and eliciting support and communication skills; (iii) Emotional: linking effect to events, and emotional regulation and processing; (iv) Cognitive: identifying thoughts, insight-building, distraction, and mindfulness.
For counselling sessions, the content was also developed keeping in mind the relevance of the instructions and guidelines to the participant’s context in terms of their socioeconomic status, livelihood, and geographical location. Thus, the modules were based on the following topics:
- Awareness: General awareness regarding Covid-19 and its symptoms, means of transmission, prevention guidelines, and potential sources of support (this is, health and relief) so as to reduce fear of infection.
- Coping with stress: Techniques of stress management, breathing exercises, and managing stressful thoughts and emotional outbursts.
- Self and childcare: Re-emphasising Covid-19-related health guidelines and advice pertaining to self-care during pregnancy, care of young children, and someone who is unwell with Covid-19-like symptoms, and information on seeking medical help during an emergency.
- Communication: Guidelines on the relevance of staying virtually connected with loved ones and neighbours, and refraining from believing or passing on unverified Covid-19 information, including not blaming or ostracising people for contracting the Virus.
We conducted a baseline survey in the rural regions of southwestern Bangladesh between May and June 2020. The survey revealed that 83% of the surveyed women had experienced moderate to severe stress during the pandemic.
To enhance their mental well-being, we designed and delivered a brief telecounseling intervention to 2,402 women residing in 357 villages in the districts of Khulna and Satkhira in southwestern Bangladesh. Participants were randomised into one of two groups: a ‘treatment group’ (those who receive the intervention) with 1,299 participants, and a ‘control group’1 (no intervention) with 1,103 participants. The counseling sessions began in mid-July 2020 on a bi-weekly basis.
Locally recruited and trained female para-counsellors, who are recent graduates in either psychology, public health, or social sciences from public universities in Bangladesh, conducted the counselling sessions. Session appointments were pre-arranged, whereby the participants could choose a convenient time. The counsellors then called the participants at their selected time. Each participant received four one-to-one telecounseling sessions. Sessions were conducted fortnightly, and each session lasted for about 25 minutes. The widespread use of mobile phones in Bangladesh makes this type of intervention possible.
We conducted two endline surveys – the first one was conducted one month after the intervention ended (November 2020), and the second one, 10 months after the intervention (August 2021)2.
Findings
After one month of the telecounselling intervention, we find that the intervention led to a 26% reduction in the incidence of moderate and severe stress and 60% reduction in depression among the treated group. After 10 months, the associated reductions were 20% and 33% for stress and depression, respectively.. We also find improvements in household-level food security, and time invested in children.
Figure 1 presents the distribution of the perceived stress scale (PSS) score on a scale of 0 to 40, and Center for Epidemiologic Studies Depression Scale (CES-D-10) on a scale of 0 to 30, for both treatment- and control-group women, with higher values corresponding to higher perceived stress and depressive symptoms among the respondents. Alternatively, when we focus on whether stress and depression are above or below a certain threshold level (that is, a person is considered stressed if her PSS score>13 and depressed if her CES-D-10 score>10), we find that the intervention led to a significant and large decline in the incidence of being stressed and depressed to the tune of 22 and 20 percentage points and 21 and 19 percentage points at the one-month endline and 10-month endline, respectively.
Figure 1. Distribution of stress and depression, by treatment status
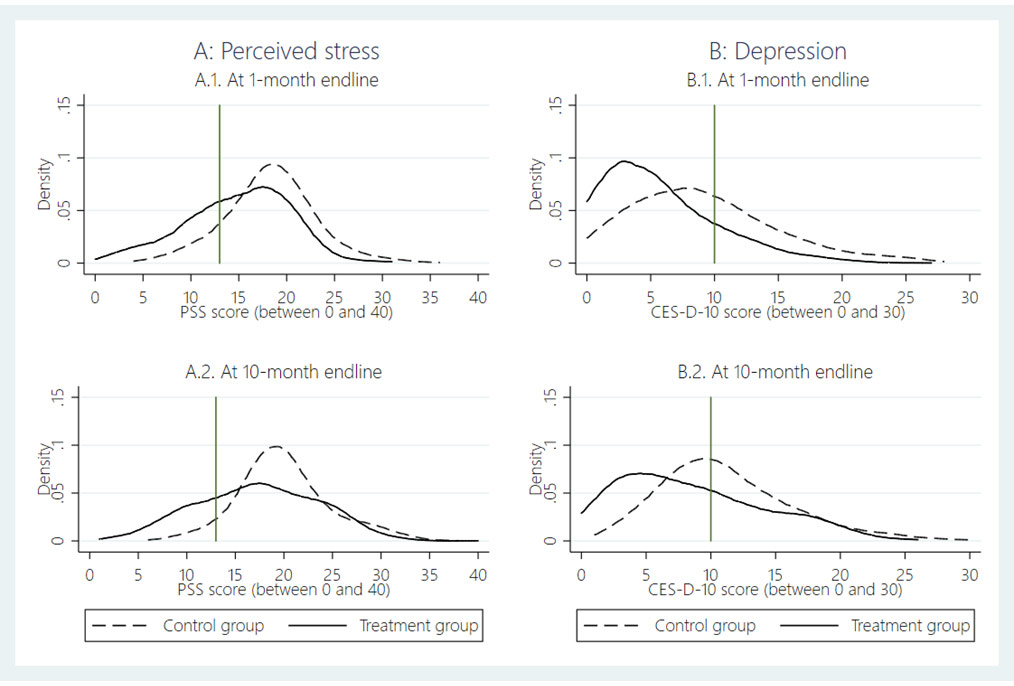
Note: The vertical line is at PSS (perceived stress scale) score 13, which is the threshold for someone being mentally stressed, and the vertical line is at CES-D-10 (Center for Epidemiologic Studies Depression Scale) score 10, which is the threshold for someone being mentally depressed.
The effect of the intervention also spills over to other outcomes beyond mental health such as, subjective well-being, preventive health behaviour, risk attitudes, social preferences, improved attitudes toward gender norms and intimate partner violence, and compliance with prescribed health guidelines related to Covid-19 prevention. Treatment group households are 6 percentage points more likely to have received at least one dose of the Covid-19 vaccine by August 2021. .
The mental health effects are stronger for women who experienced higher levels of stress to begin with, are comparatively older, and are from below median-income households. Overall, our findings suggests that a low-cost, brief telecounseling intervention can be effective in improving the mental health of women in a resource-poor setting.
Figure 2. Treatment effects in standard deviation terms, with 99% and 95% confidence intervals
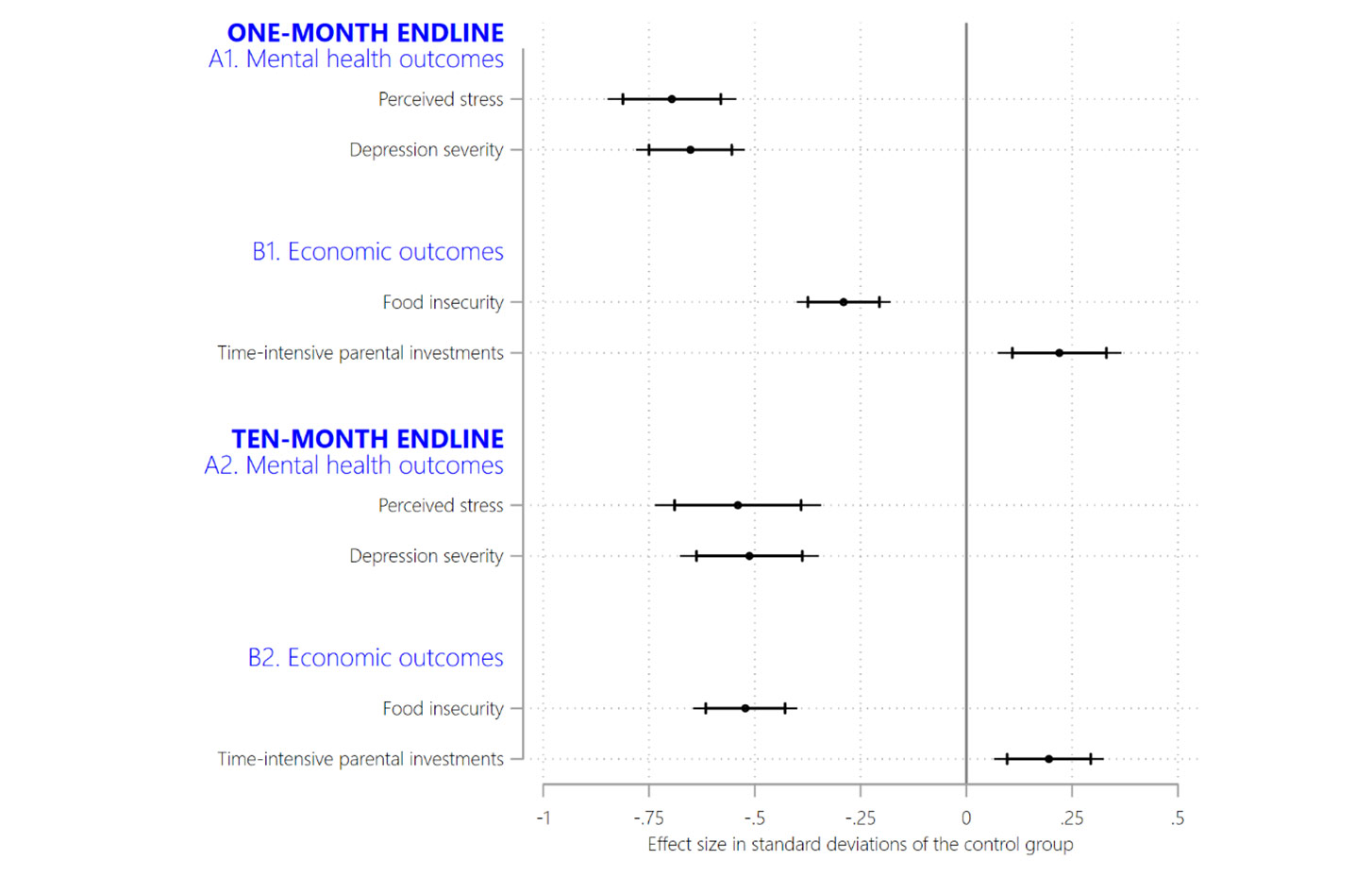
Notes: (i) Standard deviation is a measure that is used to quantify the amount of variation or dispersion of a set of values from the mean value (average) of that set. (ii) A confidence interval is a way of expressing uncertainty about estimated effects. A 95% confidence interval, means that if you were to repeat the experiment over and over with new samples, 95% of the time the calculated confidence interval would contain the true effect.
Lessons and policy implications
The telephone-delivered intervention to offer mental health support is a viable approach, as in-person counselling is not possible during the pandemic, and using video conferencing technology is not feasible in low-income and resource-poor settings. This medium enables the counselling to be delivered privately and discreetly, thus preventing recipients of mental health treatment from facing stigma. The remote and empowering nature of the intervention, coupled with the low cost of implementation, makes our intervention scalable and and it is possible to apply this to other similar contexts where providing mental health support is otherwise challenging during a crisis situation. In terms of implementation, we found some measures to be helpful. The sessions were kept short (of optimum duration) and to the point keeping in mind the daily burden of chores. The locally recruited para-counsellors were able to engage with the participants by building on their own experiences and first-hand knowledge about the lives of the women in the study area. We did not emphasise identifying participants as ‘mental health patients’, rather on empowering them with skills and knowledge to manage daily stress and negative emotions. The telephone-based intervention was thus able to reach out to participants in a cost-effective manner during this critical time, and improve overall wellbeing, without requiring them to commute or travel.
I4I is now on Telegram. Please click here (@Ideas4India) to subscribe to our channel for quick updates on our contentNotes:
- Participants in the control group (who do not receive the intervention) on average have the same baseline characteristics as the treatment groups and hence are comparable.
- In 21.6% of households in the control group, at least one adult member has received one dose of vaccine.
Further Reading
- Ahmed, Firoz, Asad Islam, Debayan Pakrashi, Tabassum Rahman and Abu Siddique (2021), “Determinants and dynamics of food insecurity during COVID-19 in rural Bangladesh”, Food Policy, 101: 102066 Available here.
- Brooks Samantha K et al. (2020), “The psychological impact of quarantine and how to reduce it: rapid review of the evidence”, The Lancet, 395(10227): 912-20.
- Chua Siew E et al. (2004), “Stress and psychological impact on SARS patients during the outbreak”, The Canadian Journal of Psychiatry, 49(6):385-90.
- Cowling, Benjamin J, Diane M W Ng, Dennis K M Ip, Quiyan Liao, Wendy W T Lam, Joseph T Wu, Joseph T F Lau, Sian M Griffiths and Richard Fielding (2010), “Community psychological and behavioral responses through the first wave of the 2009 influenza A (H1N1) pandemic in Hong Kong”, The Journal of infectious diseases, 202(6): 867-76.
- Galea, Sandro, Raina M Merchant and Nicole Lurie (2020), “The mental health consequences of COVID-19 and physical distancing: the need for prevention and early intervention”, JAMA Internal Medicine, 180(6): 817-818.
- Ho, Roger C, Melvyn W Zhang, Cyrus S Ho, Fang Pan, Yanxia Lu and Vijay K Sharma (2014), “Impact of 2013 south Asian haze crisis: study of physical and psychological symptoms and perceived dangerousness of pollution level”, BMC Psychiatry, 14(81).
- Holmes Emily A et al. (2020), “Multidisciplinary research priorities for the COVID-19 pandemic: a call for action for mental health science”, The Lancet Psychiatry, 7(6): 547-560.
- Islam, A., C. Wang, M. Vlassopoulos, and D. Pakrashi (2021) “Stigma and Misconception in the time of COVID-19 Pandemic: A Field Experiment in India”, Social Science and Medicine, 278, 113966, June 2021 Available here
- James, PB, J Wardle, A Steel and J Adams (2019), “Post-Ebola psychosocial experiences and coping mechanisms among Ebola survivors: a systematic review”, Tropical Medicine & International Health, 24(6): 671-91.
- Lund Crick, Alison Breen, Alan J Flisher, Ritsuko Kakuma, Joanne Corrigall, John A Joska, Leslie Swartz and Vikram Patel (2019), “Poverty and common mental disorders in low and middle income countries: A systematic review”, Social Science and Medicine, 71(3): 517–28. Available here.
- Mucci Nicola, Gabriele Giorgi, Mattia Roncaioli, Javier Fiz Perez and Giulio Arcangeli (2016), “The correlation between stress and economic crisis: a systematic review”, Neuropsychiatric Disease and Treatment, 12: 983-993. Available here.
- Rahman, Tabassum, MD Golam Hasnain and Asad Islam (2021), “Food insecurity and mental health of women during COVID-19: Evidence from a developing country”, PLoS ONE, 16(7): e0255392. Available here.
- Ravindran, S and M Shah (2020), ‘Covid-19: ‘Shadow pandemic’ and violence against women’, Ideas for India, 17 September.
- Stain, Helen J, Brian Kelly, Vaughan J Carr, Terry J Lewin, Michael Fitzgerald and Lyn Fragar (2011), “The psychological impact of chronic environmental adversity: Responding to prolonged drought”, Social Science & Medicine, 73(11):1593-9.
- Vlassopoulos, M, A Siddique, T Rahman, D Pakrashi, A Islam and F Ahmed (2021), ‘Improving Women’s Mental Health During a Pandemic’, Munich Papers in Political Economy Working Paper No. 02/2021. Available here.

Comments will be held for moderation. Your contact information will not be made public.