

 27 June, 2016
27 June, 2016 





The Indian population is increasingly becoming overweight or obese, and this phenomenon is likely to impose a considerable health burden in the future. Analysing data from the Indian Human Development Survey, this column finds that obesity is more evident among affluent, well-educated, urban groups, especially adult women. Increasing incomes and sedentary lifestyles are key contributing factors.
Much of the health economics literature in India has focused on the pervasive problem of malnutrition and infectious diseases. However, a topic that has garnered considerably less attention is the rising phenomenon of being overweight and obese. India currently has the third highest number of obese and overweight people in the world. On average, 5% of those below the age of 20 and 20% of those above the age of 20 fall in this category (Ng et al. 2014). These numbers are rising and are likely to impose a considerable health burden in the future. Our study examines the prevalence of being overweight and obese in a comprehensive manner, and documents patterns separately for rural and urban India (Maitra and Menon 2016).
Analysis
We use data from two rounds of the nationally representative India Human Development Survey (IHDS) to document patterns specific to adult males and females (18 years of age and above). This age group is important because it demarcates those in both the productive and reproductive age brackets. The IHDS data are apt for purposes of our study as 83% of the households from the first round (conducted in 2004-2005) were re-surveyed in the second round (2011-2012) allowing the construction of a panel that spans about seven years. Our study of adults compares men and women in 2012, and women in 2005 and 2012. Categorising adults into different weight categories based on body mass index (BMI) as per WHO (World Health Organization) cut-offs: underweight (BMI < 18.5), normal weight (18.5 < BMI < 25), and overweight or obese (BMI > 25). Figure 1 shows the proportion of males and females in each category in 2012.
Figure 1. Proportion in different weight categories by gender

While the proportion of adults that is underweight is comparable by gender, women are more likely to fall in the overweight and higher category. The patterns become even starker upon disaggregation by urban and rural residence.
Figure 2. Proportion in different weight categories by gender and rural/urban residence
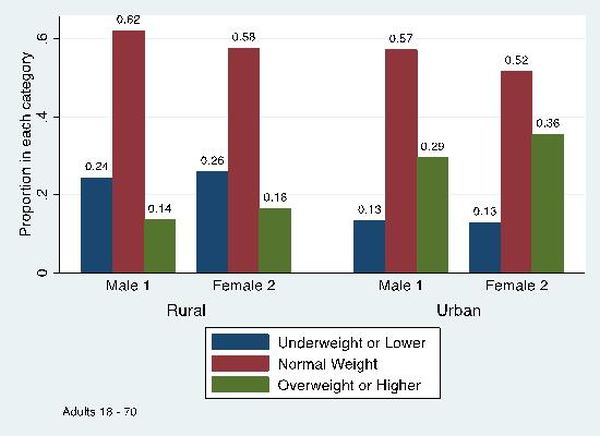
Figure 2 shows that while there is some evidence of prevalence of excess weight in rural areas, the problem is most evident in urban settings with 29% of men and 35% of women being categorised as overweight or obese. Thus, over one third of adult women in urban India (and close to a third of adult men) are overweight or obese. Focusing on the underweight category, the proportion in is significantly higher in rural settings, as expected.
Analysing patterns by gender and state of residence, shows that there is considerable variation across the country. In rural areas, rates of excess weight are highest among women in Kerala, Punjab and Jammu and Kashmir. In Tamil Nadu, Haryana and Andhra Pradesh, rates for men exceed those for women in rural settings. In urban areas, women in Punjab, Jammu and Kashmir and Haryana depict the highest rates. Estimates for urban Punjab reveal that over 50% of women are overweight or obese. In fact, the minimum rate of ‘overweight or higher’ among urban women is not less than 20% in any of the major 22 Indian states. Rates for urban men are more variable but again, are generally over 20% in the majority of Indian states.
BMI is greater for married individuals, those belonging to upper quartiles of the expenditure distribution, the more educated, and those owning a car or a motorcycle. For women, hours watching television and the presence of domestic help both increase BMI.
Figure 3. Transition matrix, Females aged 18 or higher in 2005
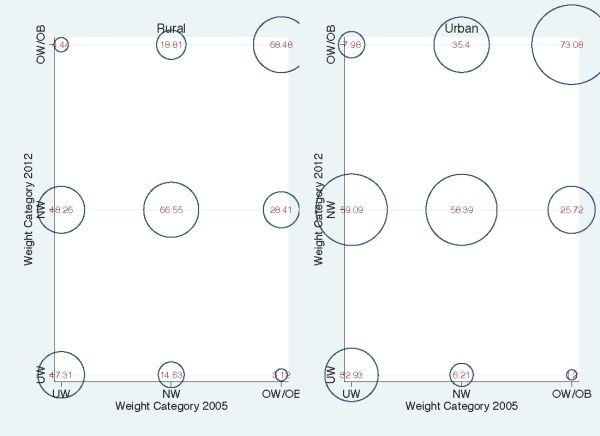
We study women who were 18 years or older in 2005 (because of data deficiencies, we are unable to follow men across survey rounds) using the panel aspect of the data. We find that the proportion of women that is overweight or obese in 2012 given that they were of normal weight in 2005 is 19%. Alternatively, 69% of those who were overweight or obese in 2005 remained in the same category in 2012. In urban areas, these proportions are even higher. Of those who were of normal weight in 2005, 35% have transitioned to the excess weight category by 2012. 73% of those who were overweight or obese in 2005 have remained so in 2012.
The main determinants of transitions from the underweight or normal weight categories in 2005 to the overweight or obese category in 2012 (including those who have remained in the excess weight capacity from 2005 to 2012) include base weight in 2005, urban residence, secondary schooling or higher, consumption expenditure per capita, salaried work, hours spent watching television, the presence of household help (only in urban areas), and share of total expenditure spent on eating outside the home (mostly in the full sample and rural areas). Although some of the variables are measured with less precision (in estimates that take account of factors we cannot measure), marriage continues to be a strong predictor of overweight or obese status for women in urban areas; BMI is systematically higher for women in households at higher expenditure quartiles, and hours spent watching television continues to be associated with significantly higher BMI.
Policy importance
One reason why this issue is of critical importance is that health implications of an overweight population can be severe. As is well documented, excess weight is significantly associated with diseases such as diabetes, high blood pressure and heart disease. The Washington Post from January 2015 notes: “Experts say India suffers from the double burden of rising obesity and diabetes. The country has about 65 million patients, and about 80% of those cases are caused by obesity.” The IHDS has self-reported measures of disease, and although these may suffer from the usual problems of misreporting and measurement error that may be systematically associated with gender and income classes, our preliminary analysis reveals that being overweight or obese has a significant impact on heart disease and diabetes.
Conclusion
Our research reveals that in addition to malnutrition, India is fast developing an overweight/obesity problem. Important correlates include income and a sedentary lifestyle. This indicates that lack of physical activity and changes in socio-cultural norms that include easier access to cheap calories (fast food, sugary carbonated drinks) are important in understanding root causes. In ongoing work, we extend this analysis to adolescents. Preliminary estimates indicate that excess weight is less evident among the youngest populations but becomes measurably apparent in secondary school with the onset of teenage. Our future research will use natural experiments to identify mechanisms that drive this phenomenon in a causal manner.
Further Reading
- Maitra, P and N Menon (2016), ‘Portliness amidst Poverty: Evidence from India’, Mimeo.
- Ng et al. (2014), “Global, Regional, and National Prevalence of Overweight and Obesity in Children and Adults during 1980-2013: A Systematic Analysis for the Global Burden of Disease Study 2013”, Lancet, 384: 766-781.

Comments will be held for moderation. Your contact information will not be made public.