

 18 August, 2020
18 August, 2020 





Besides lack of schooling resources, a possible reason why children grapple with low learning outcomes may be poor health at birth. Analysing data from Andhra Pradesh, this article finds that a 10% increase in birth weight increases cognitive test scores in mid-childhood, by 7.2%. This positive effect of birth weight on cognition is larger for boys, children from rural or poor households, and those with less-educated mothers.
In India, approximately 18% of infants were born with low birth weight during 2010-2015 (International Institute for Population Sciences (IIPS) and Inner City Fund (ICF), 2017). At the same time, despite significant increase in school enrolment, learning outcomes remain suboptimal for primary school-age children in India. For example, only 42.5% of grade 3 children were able to read grade 1 text, only 32% children in grade 2 could read simple words in English, and slightly more than one-fourth of the grade 3 children could do a two-digit subtraction (Annual Status of Education report (ASER) Centre, 2016). Besides lack of schooling resources, a possible reason why children grapple with low learning outcomes may be poor health at birth.
Birth weight and cognitive development
Low birth weight, defined as birth weight less than 2.5 kgs, remains an important public health challenge with adverse health and economic consequences for resource-poor households in developing countries. Reducing the incidence of low birth weight can increase human capital and human welfare in developing countries as studies in the high-income countries show that infants with low birth weight perform poorly on cognitive tests, attain fewer years of schooling, and earn lower income as adults (Currie and Vogl 2013).
However, very little is known about the effects of birth weight on these outcomes in low-income countries. Furthermore, much less is known about the effects of birth weight on mid-childhood cognitive outcomes, and how cognitive development evolves between birth and mid-childhood (5-8 years). Mid-childhood outcomes are important because the birth weight effects on adult outcomes manifest through the mid-childhood years and are more amenable to policy intervention compared to adult outcomes.
The effect of initial health endowment on human capital could be qualitatively different in lower-middle-income countries (LMICs) because poor schooling may prevent cognitive ability from translating into high levels of human capital. Furthermore, there may be gender and other biases in allocation of resources within the household that could attenuate the link between health at birth and human capital later in life. The effect of birth weight on human capital outcomes could depend on the intra-household allocation of resources among children with differing abilities, and parental decisions to invest resources based on their birth endowment (Almond and Mazumdar 2013). Therefore, a key question of significant policy importance is to establish causal relationship between low birth weight and cognitive abilities in developing countries because lack of causal association implies that the returns to investment in improving birth outcomes will have limited returns.
Analysing data from Andhra Pradesh
In recent research (Kumar et al. 2019), we study whether children born with low birth weight have lower test scores at age eight. We use the first three rounds (2002, 2006, 2009) of the Young Lives data from Andhra Pradesh (AP). The Young Lives survey is drawn from three distinct agro-climatic regions of AP: Coastal Andhra, Rayalaseema, and Telangana. The average birthweight in the sample is 2.763 kgs, and 17% of the sampled children were born with low birth weight. The main outcome variable is Peabody Picture Vocabulary Test (PPVT) at age five and eight, an important measure of cognitive development. The PPVT score is a widely used test to measure verbal ability and general cognitive development among children. Our sample consists of 868 children whose birth weight information was available from round 1, and the PPVT test scores were available from rounds 2 and 3.
Our analysis demonstrates that birth weight is an important predictor of PPVT test scores in Andhra Pradesh. Figure 1 shows a positive association between birth weight and test scores: as birthweight increases, PPVT scores also increases.
Figure 1. Positive association between birth weight and test scores
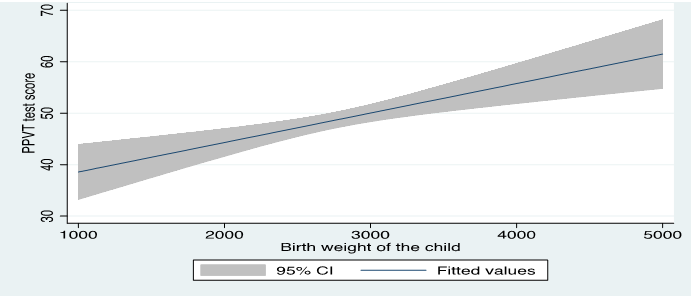
Note: 95% CI refers to 95% confidence interval. A 95% confidence interval is a way of expressing uncertainty about estimated effects. Specifically, it means that if you were to repeat the experiment over and over with new samples, 95% of the time the calculated confidence interval would contain the true effect.
The results in Figure 1 do not control for selection bias and confounding variables, and therefore, cannot be interpreted as causal effects of birth weight on tests scores. For example, if more educated parents adopt healthy behaviours that could affect birth weight and children’s education, then this simple analysis would produce biased results.
Therefore, to estimate the causal and unbiased impacts, we use maternal height and probability of premature birth as instruments for birth weight. The average mother’s height is 151.4 cm and 9% of the births were premature (born before 37 weeks). Mother’s height and pregnancy outcomes are likely to be correlated because maternal height reflect mother’s cumulative social and nutritional conditioning that may impact the intrauterine environment and thus affects birth weight; maternal height and birth weight are likely to be positively correlated. Similarly, preterm birth is a leading cause of low birth weight as premature babies have constrained growth inside the womb.
Our main findings in this study is that a 10% (276 gms) increase in birth weight increases the PPVT score by 7.2% or 0.11 standard deviations, which is an economically and statistically significant effect. Furthermore, while comparing the test scores of low birth weight and normal birth weight children, we find that low birth weight children have 65% lower test scores compared to normal birth weight children.
Variable impacts
The other question of policy relevance is whether the birth weight effects on test scores vary by the socioeconomic status and gender of the child because in addition to biological factors, parental behaviour or environmental factors may affect later-life human capital. In theory, parents may either reinforce or compensate for the low birth weight. For example, parents who prefer to compensate for poor birth endowment might invest more on low birth weight children and hence weaken the birth weight effects on outcomes. The analysis documents that the birth weight effects are larger in magnitude for rural areas, boys, the poor, and children born to less-educated mothers. These results imply that parental nurturing or investment on children may moderate the biological determinants of test scores in the mid-childhood years. However, the effect of birth weight on the test scores did not differ by household caste – scheduled caste/tribe children and those from other social groups had similar propensity to benefit from improvement in birth weight.
Another interesting finding is that the effects of birth weight on test scores are not uniform across the distribution of the PPVT scores. We find that the positive effects of birth weight vary by the quantiles of the PPVT scores; children at the lower distribution of the PPVT scores benefit more from improvement in birth weight compared with children at the higher PPVT distribution.
Conclusion and policy recommendations
These findings indicate that health endowment at birth (especially birth weight) is positively associated with test scores among school-age children in India, and that children from socially and economically disadvantaged background benefit more from improvement in health status around birth. These findings support the notion that the problem of low human capital in developing countries could be addressed by health programmes targeted to improve health outcomes at birth, including birth weight. Our findings point to the critical importance of targeted health and nutrition policies for low-income pregnant women that could improve the prenatal and in-utero environments, which would reduce the burden of low birth weight among newborns in India, and in turn, may improve human capital accumulation.
Notes:
- Outcome variable is the variable which is explained in a regression model, whose value depends on the values of one or more other variables, called the independent or explanatory variables.
- Selection bias occurs when the selection of observations from a population is not random, and therefore, unrepresentative of the population.
- Instrumental variables are used in regression analysis when the outcome and predictor of interest are determined simultaneously or when both are correlated with an omitted variable in the model. An instrument is a third variable used to identify the unobserved correlation, which allows us to see the true correlation between the predictor and outcome variable.
- Standard deviation is a measure that is used to quantify the amount of variation or dispersion of a set of values from the mean value (average) of that set.
- These findings are robust to the addition of several child- and household-level controls, and community fixed effects in the analysis.The fixed effects control for time-invariant unobserved individual characteristics.
Further Reading
- ASER Centre (2016), ‘Annual Status of Education report’, Pratham, India.
- Currie, Janet andTomVogl (2013),“Early-Life Health and Adult Circumstance in Developing Countries”, Annual Review of Economics, 5:1-36.
- International Institute for Population Sciences (IIPS) and ICF (2017),‘National Family Health Survey (NFHS-4), 2015-16’, Mumbai, India.
- Kumar, S, K Kaushalendra, RLaxminarayan and ANandi (2019),‘BirthWeight and Cognitive Development during Childhood: Evidence from India’, Global Labor Organization (GLO) Discussion Paper Series 358.

Comments will be held for moderation. Your contact information will not be made public.