

 22 April, 2022
22 April, 2022 





Vaccine hesitancy poses a threat to India’s fight against Covid-19, and given the different motivations that drive vaccine hesitancy, a one-size-fits-all solution may not be feasible. In this post, Daral and Shashidhara use data from a Facebook survey – conducted in partnership with the University of Maryland – to identify the barriers and beliefs driving vaccine hesitancy, by segmenting the vaccine hesitant into ‘personas’ based on their psycho-behavioural profiles.
In the aftermath of the third wave of Covid-19, which spread across India at a hitherto unprecedented rate, the need for universal vaccination is becoming increasingly apparent. Covid-19 vaccines have been shown to reduce the likelihood of hospitalisation by 29 times. Achieving universal vaccination is essential to reduce the risk of the emergence, and spread, of future Covid-19 variants (Rubin 2021), with vaccine hesitancy being a legitimate threat to India’s fight against Covid-19 (Umakanthan et al. 2021).
Vaccine hesitancy is grounded in a range of concerns and motivations – these include insufficient knowledge, questions around the efficacy of the vaccine, concerns about potential side effects, or a desire to ‘wait and watch’ before deciding to take the vaccine (Chandani et al. 2021). This group of individuals – often termed as ‘anti-vaxxers’ – are highly resistant to change and tend to believe in, and occasionally propagate, misinformation about vaccines (Latkin et al. 2021).
Given the different motivations that drive vaccine hesitancy, a one-size-fits-all solution may not be feasible when dealing the issue. Traditional demographic cohorts can help identify the question of ‘who’ remains unvaccinated. In contrast, segmenting individuals based on their psycho-behavioural profiles can help target people's barriers and beliefs. These ‘personas’, often used in human-centred designs (HCDs), are archetypal representations of a population and provide a snapshot of their motivations.
The study
We analyse data from the COVID-19 Trends and Impact Survey (UMD (University of Maryland) Global CTIS) (Fan et al. 2020) – a daily global survey conducted on Facebook by the University of Maryland since April 2020 – to investigate the number of personas or distinct profiles of knowledge attitudes and beliefs around Covid-19 and vaccines, in the Indian population. As of 31 October 2021, over 1.8 million Indians have responded on the social media platform on topics ranging from Covid-19 symptoms, perceptions around Covid-19-appropriate behaviours (CAB) such as mask-wearing, mental health issues, and vaccine acceptance. Using data from May-October 2021, we study over 26,000 individuals who were still unvaccinated at the time of the survey (18% of the total respondents in the time frame examined)1.
Our sample is representative of India's Facebook users and hence, is likely to be skewed towards college-educated urban males as 25% of India’s Facebook users comprise this demographic group. Of the 26,000 unvaccinated individuals, our final sample includes 10,600 “Vaccine hesitant” participants from India, that is, those who did not say they “Definitely Will” get vaccinated. This includes respondents who stated that they had not taken the vaccine nor an appointment to receive the same.
Figure 1a: Vaccine hesitancy in the study sample
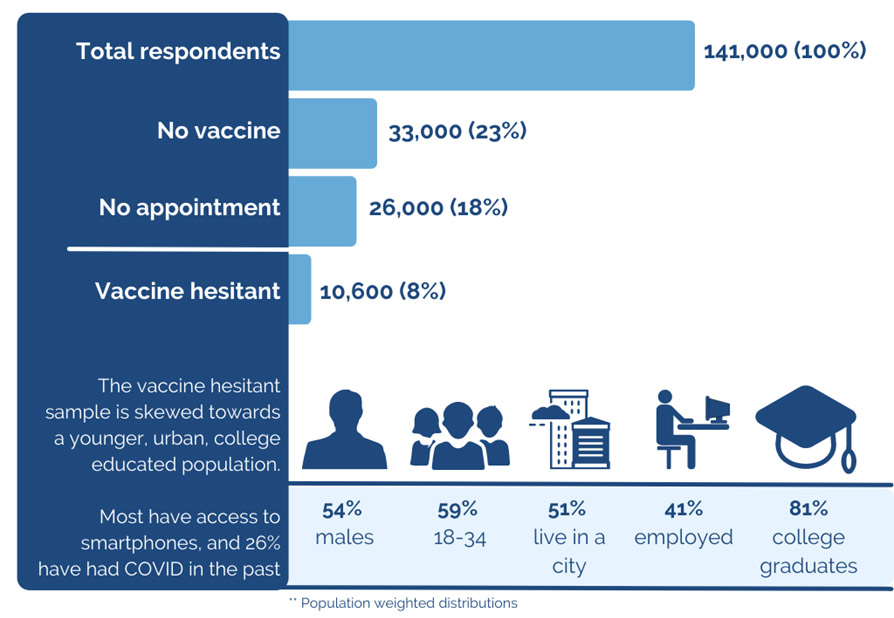
Note: Each group of respondents (No vaccine, No appointment, Vaccine hesitant) is a subset of the previous group
Figure 1b. Intent to get vaccinated
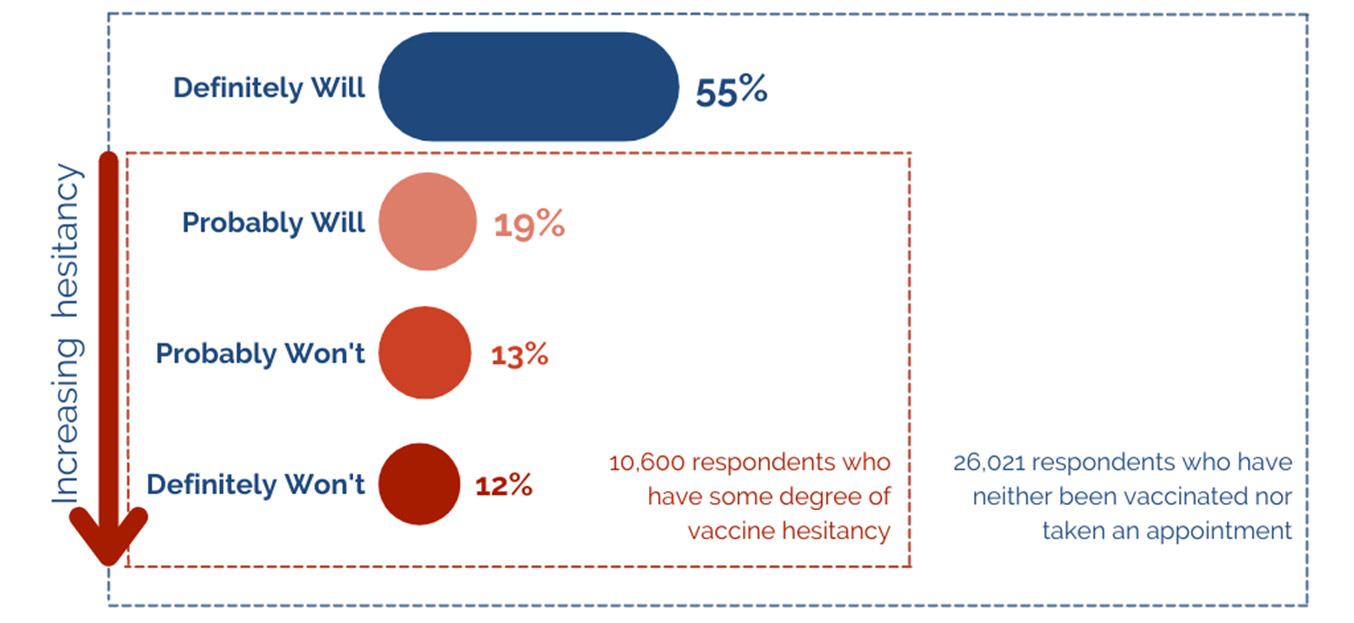
Note: The above figure includes responses (of those in the “No appointment” group from Figure 1a) to the question “If a vaccine to prevent COVID-19 (coronavirus) were offered today, would you choose to get vaccinated?”.
Defining hesitancy based on intent to get vaccinated, we find that around 45% of the individuals who are currently unvaccinated have some degree of hesitation. We segment2 this smaller sample into vaccine hesitancy personas based on 16 attributes. These assess their intent to get vaccinated, barriers to vaccination, attitudes towards CABs, level of worry because of Covid-19, trust in sources and channels for Covid-19-related information, and belief in misinformation. These 16 characteristics, weighted by geographic population, make seven different personas, and provide significant insights into the decision-making process of the unvaccinated.
Vaccine hesitancy personas
Our results3 show seven distinct personas in the population: (i) Afraid (but willing), (ii) Confused, (iii) Apprehensive, (iv) Complacent, (v) Indifferent, (vi) Sceptical, and (vii) Anti-Vaxxers.
“Afraid (but willing)” include those who are pro-vaccination but are hesitant primarily due to concerns around vaccine side effects and/or efficacy and would rather wait before getting the vaccine themselves. They believe in the effectiveness of CABs and worry about their health during Covid-19. Those who are “Confused” have a steadfast belief in the effectiveness of CABs and trust multiple sources for their Covid-19-related information. However, they are less concerned about vaccine side effects and efficacy, with no single significant barrier to vaccination. The “Apprehensive” prefer to wait and watch, mainly due to lower trust in Covid-19-related information sources. They are not concerned about side effects or vaccine efficacy. The “Complacent” cohort thinks others need the vaccine more, are concerned about vaccine side effects but do not see it as a barrier, and do not have religion-related concerns, or doubts about its efficacy.
Those “Indifferent” do not have a specific reason for remaining unvaccinated – they are not concerned about side effects, do not strongly believe that the vaccine is ineffective or follow a wait and watch strategy, and they do not believe other people need it more. Those in the “Sceptical” group show less consideration for CABs, have a lower perceived severity of illness of Covid-19, are not particularly concerned about side effects, have very low intent to get vaccinated, and are highly prone to believing in misinformation. Anti-vaxxers are anti-vaccination – they do not think the vaccine is effective, do not believe they need one, and express displeasure towards the vaccine in general. They express low intent to get the vaccine and cite ‘other people needing it more’ as a barrier to getting vaccinated themselves.
Table 1. Demographic and regional variations across the seven personas
|
Persona |
Demographic variations |
Regional variations |
|
Afraid (but willing) |
Representative of Facebook user base |
Exceeds national average in the states in Northeast India, Delhi, Goa, and Tamil Nadu |
|
Confused |
Older, lower likelihood of being college-educated |
Exceeds national average in Bihar and Kerala, and lower than national average Delhi and Karnataka |
|
Apprehensive |
Representative of Facebook user base |
Exceeds national average in north India, particularly Punjab, Jammu and Kashmir, Himachal Pradesh, and Haryana; and Telangana in South India |
|
Complacent |
Younger, lower likelihood of being college-educated |
Exceeds national average in Uttar Pradesh, Haryana, Telangana, and Andhra Pradesh |
|
Indifferent |
Higher likelihood of having had Covid-19 in the past, being non-urban and college-educated; more likely to be women; and more likely to have had prior Covid-19 infections. |
Exceeds national average in Himachal Pradesh, Uttarakhand, Gujarat, and Jharkhand. Lower than national average in states in Northeast India, and Bihar. |
|
Sceptical |
Older, lower likelihood of having had Covid-19 in the past, and being college-educated; more likely to be men; and higher likelihood of being non-urban. |
Exceeds national average in Odisha, Gujarat, Chhattisgarh, Punjab, and Rajasthan. |
|
Anti-vaxxers |
Lower likelihood of being college-educated, and more likely to be men. |
Exceeds national average in Madhya Pradesh, Uttarakhand, and Rajasthan. |
We find that vaccine hesitancy is multi-faceted, driven by differences in knowledge, attitudes, and beliefs about Covid-19 and the vaccine. The most significant section of the hesitant population (30%) are “Afraid (but willing)”, that is, showing mild levels of hesitancy and are mostly concerned about side effects. Only 4% comprise the most hesitant group, the “Anti-Vaxxers”, who don't believe the vaccine is required.
Figure 2a. Key indicators and their ranking across personas
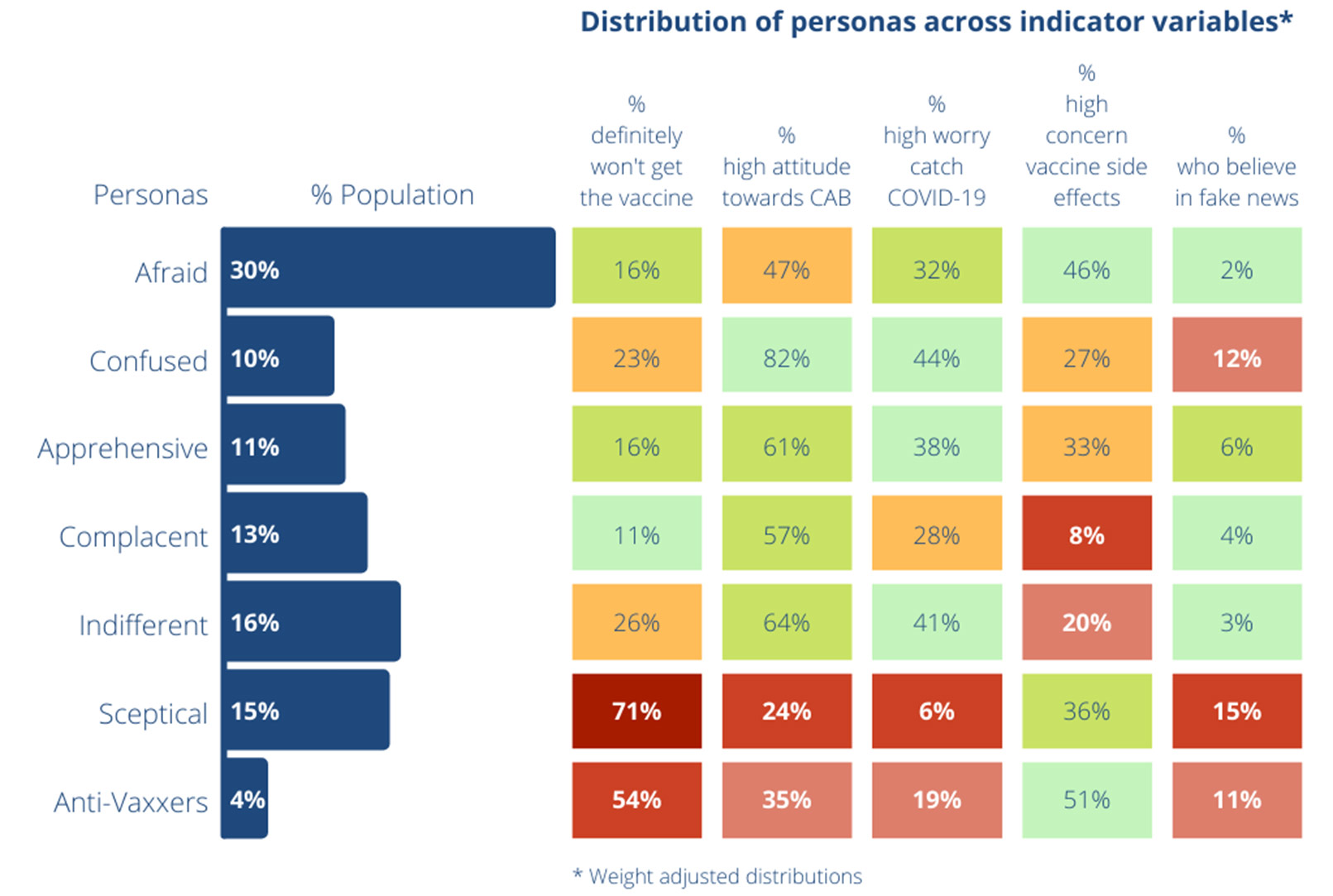
Note: Red, yellow, and green highlights indicate rankings, that is, how well a persona does within each indicator. Green signifies a better relative performance in the respective indicator, while red signifies that the persona has a relatively low score in that indicator.
Figure 2b. Seven personas and suggested intervention strategies based on key barriers
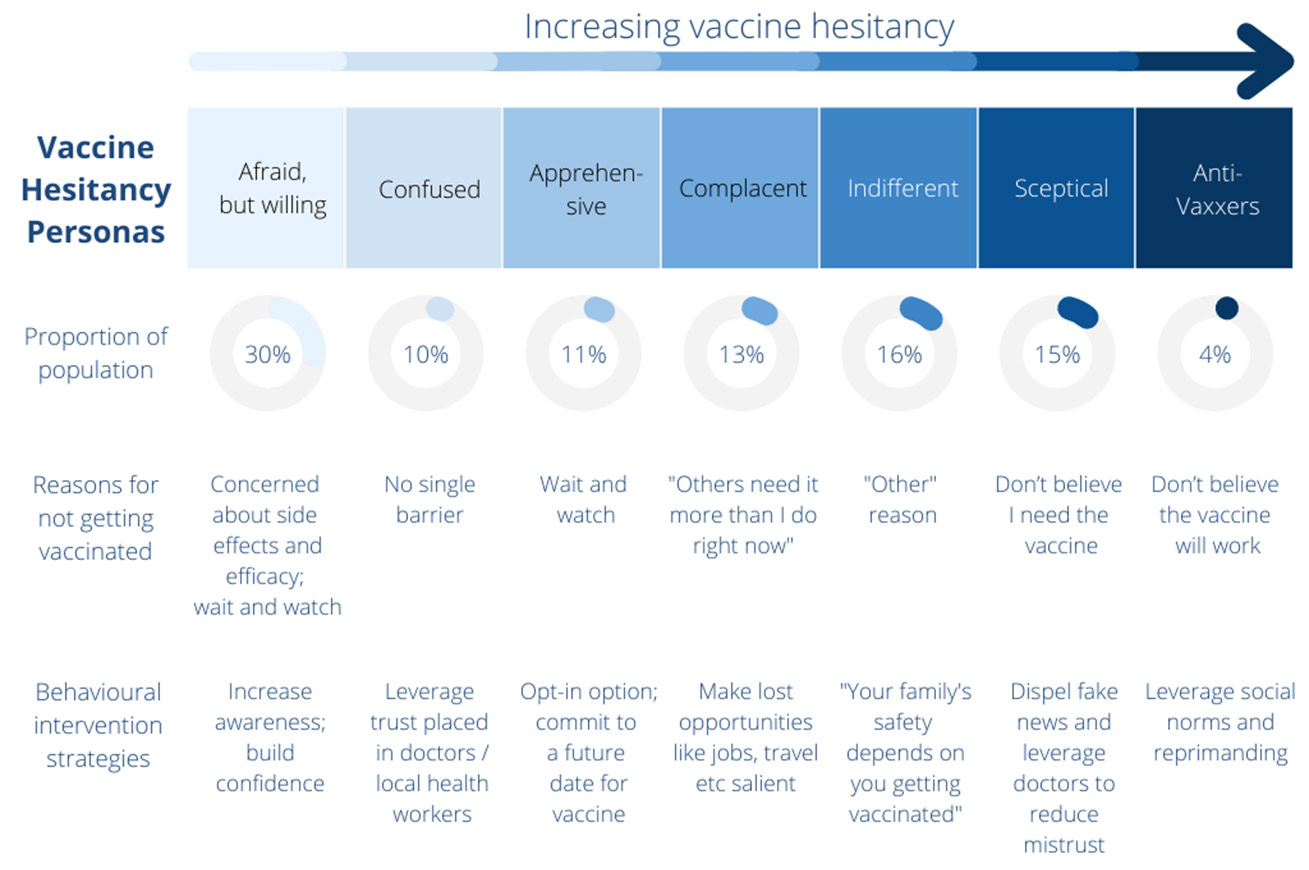
Figure 3. Weight-adjusted distribution of personas across states
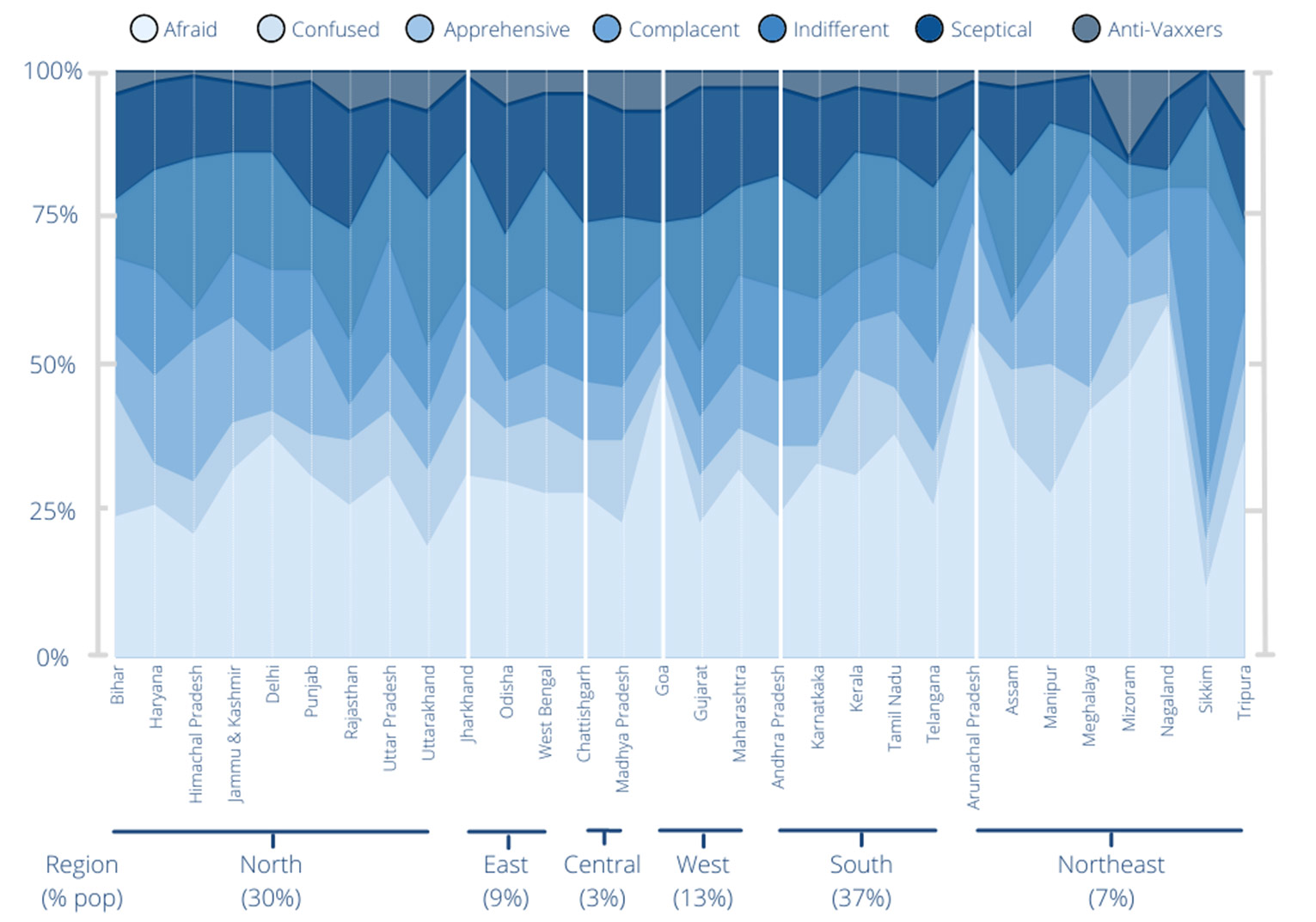
Note: Results reflect a broadly similar distribution across states except for the Northeast, which is not interpreted further due to the small sample size.
Figure 4. Weight-adjusted distribution of personas across age groups, area, and gender
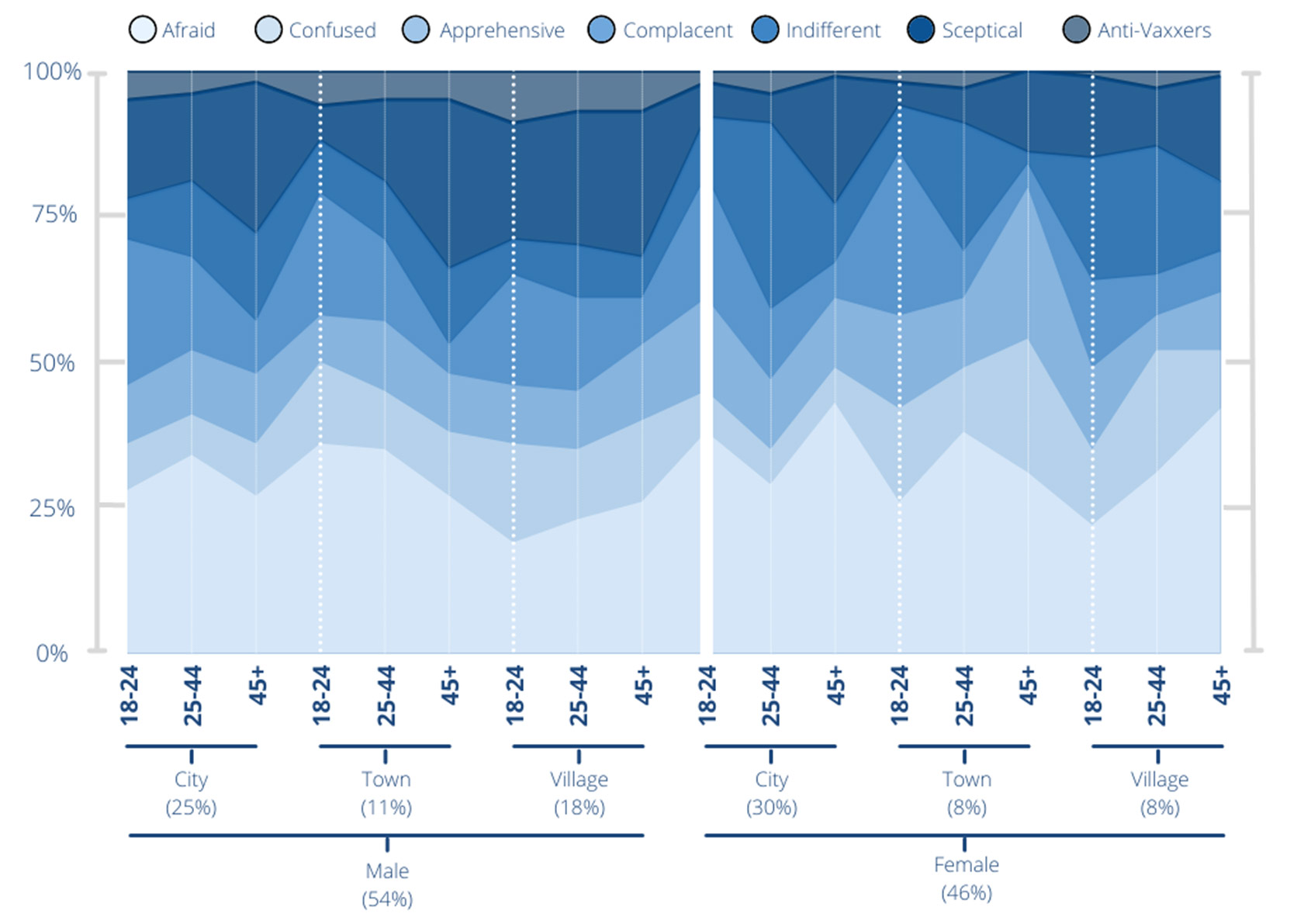
Note: There are minor differences in the distribution across the different types of groups. Importantly the high hesitancy personas are not over-represented in any one demographic.
Several studies examining hesitancy regarding Covid-194 and other vaccines5 have also used personas – based on people's behaviour and attitudes and not just demographic details – to have a clearer picture of the drivers of vaccine hesitancy. It is imperative that we examine and document the unique points of view people have regarding vaccinations, an issue that involves their health and finance, society's healthcare systems, and national and local policies. Due to the complex nature of vaccine hesitancy, any messaging aimed at counteracting hesitancy should also be tailored to their specific mindsets.
Targetted messaging based on personas
Given the characteristics of the “Afraid (but willing)” persona, campaigns should focus on increasing awareness and building confidence about the safety and efficacy of the vaccines, and highlight the alternative, that is, having a higher likelihood of serious illness on contracting Covid-19 if unvaccinated, as being more dangerous and expensive. Side effects should be framed as being a natural outcome of vaccinations, and even an indication that the vaccine is working. At the same time, people should also be nudged to plan their personal and professional work, taking into consideration the downtime that may be needed on account of the side effects. For the “Confused” persona, their trust in doctors and local healthcare workers can be leveraged to increase awareness, and also to increase how much they value the vaccine. Trusted sources should be leveraged to support these individuals’ decision-making regarding taking the vaccine. Behavioural science suggests that people prefer a ‘compromise’ over an extreme option when undecided. Since the “Apprehensive” like to wait and watch providing them with an opt-in opportunity and asking them to commit to a future date for a Covid-19 vaccine appointment may help reduce their hesitancy. It should be stressed that a return to 'normal' is less achievable with more unvaccinated people in the population. Restrictions and lockdowns are more likely to continue if more people wait to get vaccinated. The “Complacent” feel other people need it more, and hence, asserting their social responsibility is paramount when communicating with them. Covid-19 is highly infectious, and it should be emphasised that along with protecting vulnerable people by providing them with the vaccine, we all need to get vaccinated to arrest the spread of Covid-19. The “Indifferent” may not have a specific barrier to being vaccinated and therefore, we suggest an emotional approach – “your family's safety depends on you getting vaccinated”. It is worth emphasising that a prior Covid-19 infection does not reduce the need to get vaccinated.
Sceptics could benefit from a two-pronged approach: On the one hand, they need to be provided with critical facts to dispel misinformation. On the other hand, these facts need to be delivered by trusted experts such as local frontline health workers or personal doctors to reduce mistrust. In this case as well, vaccination has to be emphasised as necessary to be able to return to 'normality'. However, anti-vaxxers may respond better to being incentivised to conform with social norms. It may be useful to leverage social sanctions and reprimands by local communities on those not following Covid-19-appropriate protocols, along with some form of positive reinforcements from their peer group for getting vaccinated.
While we need to address the specific demand-side issues these populations face, supply-side issues also need attention. Those who were unvaccinated but not 'opposed' to the vaccine in our sample, reported problems with vaccine availability, lack of availability of convenient appointment slots, technical difficulties with the CoWIN website, difficulties in travelling to the vaccination centre, and getting time off from work or school to take the vaccine and recover from side effects, more often than those vaccinated. Most of these problems are likely to have been resolved with vaccines now being more widely available vis-à-vis May-July 2021. However, employers granting paid time off for taking the vaccine and recovering can go a long way in making the process convenient and incentivise vaccination.
Conclusion
To achieve universal vaccination, health officials should accurately identify who to reach, and more importantly, how to get through to them based on their psychological make-up. Successful Covid-19 vaccine communication would need to acknowledge the diversity of barriers in the unvaccinated population and plan accordingly. Our study identifies seven vaccine hesitancy personas using a broad array of psychological constructs to aid future public health messaging. Given the differences in the knowledge, attitudes, and beliefs in the different vaccine hesitant groups, messaging in this regard should be tailored to these groups. Employing behavioural science can help policymakers reach these groups more effectively.
Notes:
- As per government regulations, the 18-44 age group became eligible for vaccinations from 1 May 2021.
- We use a probabilistic Latent Class Model (LCM) for this segmentation. An LCM is a statistical procedure used to identify qualitatively different subgroups within populations who often share certain outward characteristics. More specifically, it’s a way to group subjects from multivariate data into “latent classes” – groups or subgroups with similar, unobservable, membership.
- We employ stress testing to find the statistically optimal solution.
- FinalMile Consulting shows four different personas in India using a qualitative approach with a sample of 40, based on a survey conducted in January-February 2021. Their results based on the personas: “Confused, Complacent, Indifferent, and Skeptical”, align with our results. SurgoVentures identify five psycho-behavioural personas in the US using large-scale survey data: “Enthusiasts, Watchful, Cost-anxious, System-distrusters, and COVID Skeptics”. They further quantify the distribution of these personas in each state using the same UMD Facebook survey data as we use.
- Studies have also used personas to understand hesitancy about other vaccines, such as the HPV (Human papillomavirus) vaccine (Massey et al. 2021).
Further Reading
- Barkay, N, C Cobb, R Eilat, T Galili, D Haimovich, S LaRocca, K Morris and T Sarig (2020), ‘Weights and Methodology Brief for the COVID-19 Symptom Survey by the University of Maryland and Carnegie Mellon University, in partnership with Facebook’, arXiv Working Paper (arXiv:2009.14675).
- Chandani, Sneha, Deepti Jani, Pratap Kumar Sahu, Udichi Kataria, Shailendra Suryawanshi, Jagdish Khubchandani, Sanket Thorat, Sohan Chitlange and Dharmendra Sharma (2021), “COVID-19 vaccination hesitancy in India: State of the nation and priorities for research”, Brain, Behavior, & Immunity-Health, 18: 100375. Available here.
- Fan et al. (2020), ‘The University of Maryland Social Data Science Center Global COVID-19 Trends and Impact Survey, in partnership with Facebook’.
- Latkin, Carl A, Lauren Dayton, Grace Yi, Arianna Konstantopoulos and Basmattee Boodram (2021), “Trust in a COVID-19 vaccine in the US: A social-ecological perspective”, Social science & Medicine, 270: 11368 Available here.
- Massey, Phillip M et al. (2021), “Development of Personas to Communicate Narrative-Based Information About the HPV Vaccine on Twitter”, Frontiers in Digital Health, 3.
- Rubin, Rita (2021), “COVID-19 Vaccines vs Variants—Determining How Much Immunity Is Enough”, JAMA, 325(13): 1241-1243.
- Umakanthan, Srikanth, Sonal Patil, Naveen Subramaniam and Ria Sharma (2021), “COVID-19 vaccine hesitancy and resistance in India explored through a population-based longitudinal survey”, Vaccines, 9(10): 1064.

By: Sakshi 22 April, 2022
Really good article, detailed explanation on reasons of vaccine hesitancy. At the national level, focussing on the largest group of 'Afraid' would make a good start. While states can choose specific strategies related to their demographic. I can also see healthcare institutes adopting a mix of these strategies at the grassroot level based on the individual concern of the person. Something that healthcare professionals and organizations should also consider.