

 21 March, 2016
21 March, 2016 




Cash transfers to the poor, conditional on use of particular public services, are a popular tool to increase healthcare utilisation. This column evaluates the impact of one such scheme – Janani Suraksha Yojana - and finds that it encouraged pregnant women to deliver babies at healthcare facilities. It also suggests that the marginal effect of cash incentives is larger when provided to healthcare workers rather than mothers.
Every year over 300,000 newborns in India die the day they are born, accounting for 29.5% of such deaths globally. Primary causes of neonatal deaths1 are premature birth, low birth weight, neonatal infection, birth asphyxia , trauma, and tetanus. Curbing high rates of neonatal mortality with existing healthcare infrastructure is a key challenge for policymakers. Access to healthcare facilities, where expecting mothers are assisted by medical personnel providing pre- and post-natal healthcare, may improve neonatal survival. However, demand and supply-side factors such as financial constraints, lack of knowledge about available services, distance to medical facilities, and low quality of services limit the use of maternal healthcare services. In 2005, nearly 70% of rural women in India delivered babies at home.
Conditional cash transfers
Cash transfers to low-income households, conditional on the use of particular public services, is a popular tool to increase healthcare utilisation. A subsidy on healthcare utilisation may allow a first-time user to learn about the characteristics of that product or service, affecting his/her future demand. Latin American countries have used such Conditional Cash Transfer (CCT) programmes for a long time to improve school attendance, healthcare use, and nutritional support. Bolsa Família2 in Brazil and Oportunidades 3 (now rebranded as Prospera) in Mexico are among the most successful ones. Drawing from the success of these programmes, CCTs are increasingly becoming popular among policymakers for tackling low school attendance, nutritional deficiencies and low preventive healthcare use. By 2011, CCTs had spread to 18 countries in Latin America and covered as many as 129 million beneficiaries4. Such programmes are not restricted to developing nations alone. For example, New York City implemented Opportunity NYC in 2007 that provided cash incentives to families if a student had 95% attendance, parents attended parent-teacher meetings, and so on. Overall effects of these programmes are positive on relevant outcomes.
Advocates of CCT programmes often argue that under-investment in health and education is common if families do not readily understand their benefits, which can be addressed by the conditions imposed on the receipt of welfare schemes. CCTs are politically feasible as middle- and upper-class voters are not the direct beneficiaries of such programmes. However, the marginal contribution of the conditions added on to cash transfers are not well understood in many countries. Furthermore, verification of the statutory conditions required to receive the benefits may strain the administrative capacities in poorer countries where facilities are less developed than the Latin American countries.
Janani Suraksha Yojana
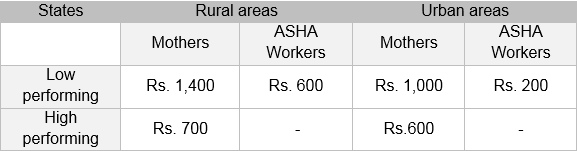
Janani Suraksha Yojana (JSY) or the Safe Motherhood Scheme is a CCT programme in India that was launched in April 2005 with the objective of improving maternal and neonatal health by promoting births in healthcare institutions5. The programme provides cash incentives to pregnant women and healthcare workers to facilitate births in public or private healthcare facilities. Eligibility for cash assistance varies by state domicile, caste, and economic status. In 10 states 6 with low rates of institutional delivery (called ‘low-performing states’), all women are eligible. For the remaining states, eligibility is restricted to two live births for women aged 19 and above and belonging to Below Poverty Line (BPL), Scheduled Castes (SC), or Scheduled Tribes (ST) households. The scale of cash assistance also varies by state and area of residence.
Table 1. Incentive amounts for mothers and ASHA workers under Janani Suraksha Yojana
 Source: Data from Quarterly National Rural Health Mission Management Information System report.
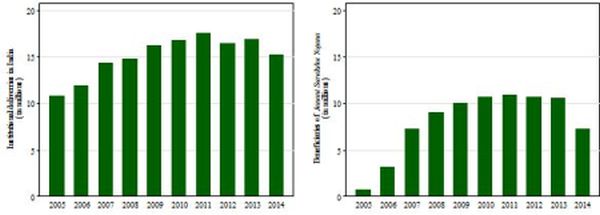
Source: Data from Quarterly National Rural Health Mission Management Information System report. Figure 1. Number of institutional deliveries and beneficiaries of Janani Surakshya Yojana (2005-2014)
 Source: Data from Quarterly National Rural Health Mission Management Information System report.
Source: Data from Quarterly National Rural Health Mission Management Information System report. Evaluation
A comparison of outcomes between the beneficiaries and non-beneficiaries of JSY to evaluate the effectiveness of the programme is appealing due to its simplicity but it would be erroneous to do so. Beneficiaries and non-beneficiaries vary along several dimensions. As long as these dimensions are visible, such as caste and possession of BPL cards, one can account for them and evaluate the programme effectively. But often factors that are not visible/quantifiable but determine both programme eligibility and use of healthcare, create errors in the evaluation of the programme.
To address these issues, I first compare the healthcare utilisation practices for women who were eligible for JSY before and after the programme. Effectively, this measures the effect of the programme and other factors that changed at the onset of JSY for eligible women. Second, I estimate the same for women ineligible for JSY, measuring the effects of other factors that changed concurrently with JSY but were not confined to eligible women. Finally I compare the pre-post differences of eligible women with that of ineligible women to find the effects of JSY.
Findings
Using data from the District Level Health Survey-III (DLHS-III) (2007-08), I find that the programme raised the likelihood of all eligible women delivering in a health facility by 4 percentage points (conservative estimate). The effects of the programme took some time to emerge, with small effects apparent in the first two years (2005–2006) and an increase of 7.2% in institutional delivery in the following two years. These effects were greater in rural areas, where the cash incentive amounts were larger for both mothers and health workers compared with that in urban areas.
Figure 2. Effects of Janani Surakshya Yojana on maternal healthcare utilisation
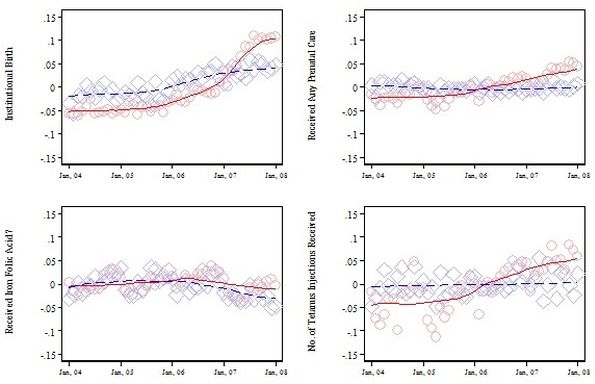 Note: Blue dotted line depicts JSY eligible and red line depicts JSY ineligible.
Note: Blue dotted line depicts JSY eligible and red line depicts JSY ineligible.Source: Author´s calculations using DLHS-III (2007-08) data.
The programme also significantly increased the probability of eligible women receiving iron-folic acid supplements, prenatal care visits, tetanus injections, and a variety of immunisations for their babies. I also found that an additional Rs. 100 incentive to ASHA workers increased the probability of an institutional delivery by 1.2 percentage points in 2007-08, with much smaller effects resulting from giving an extra Rs. 100 to mothers. The incentive effects for workers are also larger for the measures of prenatal care utilisation and immunisation. Most importantly, the programme reduced early neonatal mortality rate by four deaths per 1,000 live births, but had little impact on late neonatal mortality. These results are consistent with the increase in institutional deliveries as health institutions are more efficient in addressing complications during or immediately after childbirth as compared to births at home.
The effects of the programme varied with household income and also the level of awareness about government health programmes. The programme was most effective for relatively rich households. However, there was an increase of 2.7 percentage points in institutional delivery for poorer households when healthcare workers were also incentivised. Meanwhile, for women with relatively less information on government health programmes, JSY increased the probability of institutional delivery by 4.3 percentage points when the healthcare workers were also incentivised along with the mothers. These results suggest that the complementarities between the incentive given to the mothers and healthcare workers are strong, especially for poorer or less-informed households.
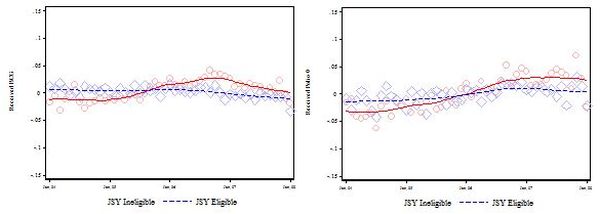
Figure 3. Effects of Janani Suraksha Yojana on Iimmunisation Source: Authors’ calculations using DLHS-III (2007-08) data
Policy implications
I find that JSY was effective in encouraging pregnant women to deliver their babies at healthcare facilities. It also improved use of other maternal healthcare services and immunisation of babies leading to fewer early neo-natal deaths per 1,000 live births. Following these results one might conclude that the CCT programme in the context of maternal healthcare was successful.
Perhaps a more intricate question is finding the optimal design of incentives for a CCT programme. Incentives can be awarded directly to the beneficiaries, conditional on utilisation, boosting demand for certain public services; or to public service providers, which can improve the quality of the services; or a combination of both. My analysis shows that marginal effects of cash incentives are larger when they are provided to the healthcare workers.
I find that the effects of the programme are significantly higher for women who are relatively more knowledgeable about other government programmes. This result supports that information plays an important role in the use of healthcare services. Additionally, my findings suggest strong complementarities between incentives for mothers and healthcare workers. However, the poorest women do not benefit from all aspects of the programme suggesting failure of targeting.
A version of this column first appeared in ISBInsight.
Notes:
- A neonatal death is defined as a death during the first 28 days of life. An early neonatal death is defined as a death during the first week of life.
- Bolsa Familia is a social welfare programme of the Brazilian government, which provides financial aid to poor Brazilian families; if they have children, families must ensure that the children attend school and are vaccinated. The programme attempts to both fight poverty by increasing human capital among the poor through conditional cash transfers.
- Oportunidades (now ‘Prospera’) is the principal anti-poverty programme of the Mexican government. It focuses on alleviating poverty in rural and urban communities through long-term investments in education, health and nutrition. By providing cash transfers to households (linked to regular school attendance and health clinic visits), the programme also fulfills the aim of alleviating current poverty.
- See Lagarde et al. (2007) for a survey of literature assessing the effects of CCTs on the use of health care facilities.
- The idea of cash transfers to recent mothers is not new in India. JSY is essentially a modification of an earlier programme called the National Maternity Benefit Scheme (NMBS) under implementation since 1995. Under NMBS, all women above the age of 19 eligible for a BPL card were given a one-time transfer of Rs. 500 for the first two births. Cash transfer under NMBS was unconditional and not tied to institutional deliveries. The genesis of this programme was from a food security and maternal nutrition perspective as opposed to healthcare service use. JSY was part of a much larger National Rural Health Mission (NRHM) that was also launched in 2005 and included the provision of patient welfare committees, grants to sub-centres, healthcare contractors, mobile medical units, ambulatory services, mother and child health wings, etc.
- Ten low-performing states where all women are eligible for JSY are Uttar Pradesh, Uttarakhand, Madhya Pradesh, Chhattisgarh, Rajasthan, Bihar, Jharkhand, Orissa, Assam, and Jammu and Kashmir.
- Accredited social health activists (ASHAs) are community health workers instituted by the Ministry of Health and Family Welfare as part of the National Rural Health Mission.
- Interestingly, the incentive amounts for ASHA workers vary by state and area of residence only for JSY.
Further Reading
- Lagarde, Mylene, Andy Haines and Natasha Palmer (2007), “Conditional Cash Transfers for Improving Uptake of Health Interventions in Low- and Middle-Income Countries: A Systematic Review”, The Journal of the American Medical Association, 298(16):1900–1910. Available at http://apps.who.int/rhl/effective_practice_and_organizing_care/SUPPORT_JAMA_cash_.pdf.

Comments will be held for moderation. Your contact information will not be made public.