

 23 August, 2017
23 August, 2017 





Political decentralisation and female representation in governance are known to improve social welfare by influencing policy decisions in favour of women and children. Analysing data from rural Bihar, this column finds that having a female leader at the village council level has a strong positive association with institutional births, and child survival rates for richer households.
Political decentralisation and female representation in governance are known to improve social welfare by influencing local policy decisions in favour of women and children (Chattopadhyay and Duflo 2004, Bhalotra and Clots-Figueras 2014). The 73rd amendment of the Indian Constitution in 1992 paved the way for political decentralisation, and mandated that at least one-third of the panchayat (village council) seats shall be reserved for women in order to enhance participation of women in local governance at the grassroots level. The eastern state of Bihar was the first to reserve 50% of seats for women - 17% more than the stipulated 33% seats – in the second panchayat election conducted in 2006. Bihar held its first panchayat election in 2001 after a gap of almost 22 years. In recent research (Kumar and Prakash 2017), we examine the impact of political decentralisation and women reservation on institutional births and child mortality in rural Bihar.
At present, there is not a lot of research on the relationship between women reservation in local governance and health outcomes in low- or middle-income countries. The evidence is especially limited in terms of the impact of greater political reservation of women on health outcomes of women and children. This study aims to fill this gap by exploring whether female leaders at the panchayat level effectively improve health outcomes in Bihar. To explore this, we assess the impact of the policy change (political decentralisation and women reservation) by comparing the health outcomes before and after the policy change in the 'treated' state of Bihar and the 'control' state of Jharkhand (where the policy was not implemented). To isolate the effects of this policy, we need a counterfactual state that would have been similar to Bihar in the absence of the reservation policy. The creation of Jharkhand from Bihar in 2000 simulates a natural experiment, making it an optimal counterfactual state to study the effects of this policy.
Studying this question in Bihar is important from a policy perspective for three reasons. First, Bihar performs poorly on several measures of human development. Second, women representation in the first panchayat election in 2001 was very low compared to other states as less than 1% of women were elected as panchayat head despite the constitutionally mandated provision of 33% (Bihar did not implement women reservation in 2001 panchayat election). Third, many argue that gender reservation in local governance may have resulted in elite capture of local resources and institutions (Bardhan et al. 2010). In this scenario, one would not expect to see improvement in delivery of public services or improvement in health or education sector because greater influence of elites in resource allocation and decision-making is likely to reduce social welfare. In this context, it is of policy interest to examine how Bihar has fared under female leaders in the politically decentralised regime after 2001.
Effects of gender quotas
Using the first (1998-99) and third waves (2007-08) of District Level Household Survey (DLHS), we estimate the effects of political decentralisation and women reservation on institutional births, safe births, and child mortality. We find that decentralisation and gender quotas in Bihar have increased institutional births, thus increasing the safety of child delivery.
The rate of institutional births in Bihar increased from 14.9% in 1998-99 to 27.6% in 2007-08. However, this increase cannot be attributed to the reservation policy because the institutional births also grew from 12.7% to 17.6% in the control state of Jharkhand during the same time period. After adjusting for socioeconomic characteristics of households and time trend captured by the increase in rate in Jharkhand, we estimate that institutional births increased by 6.5 percentage points in Bihar due the policies enacted in 2001.
Figure 1. Impact of policy on place of births, 1998-99–2007-08
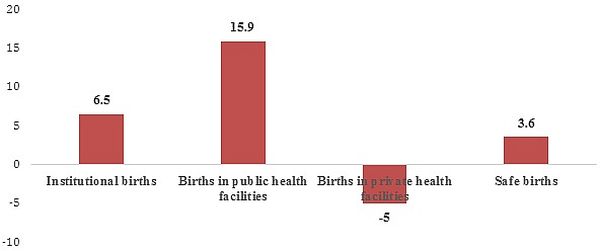 Notes: Results in figure 1 are from estimation of difference-in-difference regression models.
Notes: Results in figure 1 are from estimation of difference-in-difference regression models. We further find that the increase in institutional births was largely driven by increase in births at public health facilities rather than private health facilities: births at public health facilities increased by 16 percentage points while those in private health facilities fell by 5 percentage points in Bihar. It seems that the reservation policy was instrumental in shifting births away from private to public health facilities.
Safe delivery is another important indicator of improved maternity care and is effective in reducing maternal and child mortality. Safe delivery is defined as delivery conducted in a health facility or at home assisted by a trained health professional. On average, the rate of safe delivery increased by 10% between 1998-99 and 2007-08, of which 3.6 percentage points may be attributed to the reservation policy.
Overall, our findings show that there was a significant shift in births towards public facilities and the policy had a positive impact on the probability of safe deliveries.
When examining the relationship between women reservation and child mortality, we find that the policy change had insignificant effect, on average. However, this relationship varies across wealth groups: reservation policy reduced infant and under-five mortality in richer households but no such mortality effects were found in middle or poor households. The differential mortality effects by wealth groups is indicative of elite-capturing which implies that wealthier and powerful households are better positioned to capture the benefits of public resources relative to resource-poor households. Furthermore, poor households are slow to process information efficiently, and find it difficult to change their health behaviour quickly in response to policy change.
Concluding remarks
Our results indicate that political decentralisation and reservation of panchayat seats for women led to increases in institutional births in Bihar, particularly, births in public health facilities. These policies also led to reduction in infant and under-five mortality but only in richer households. The mortality effects were insignificant for children belonging to poor households.
There are several mechanisms through which women reservation could impact institutional births, child mortality, or other health outcomes. One hypothesis is that female leaders positively affect access and quality of services provided in public facilities. Since women and children share higher burden of health risk, female leaders are more likely to invest in health infrastructure, thus improving access and quality of health services in their regions. In addition, female leaders can have positive impacts on demand for health services by women through role-model effect. A role-model effect underscores the importance of attitudes and ambitions and implies that female leaders are effective in motivating women, changing their attitudes, perceptions, and demand for social services. Women leaders are able to influence and motivate other women to push for reform in social services.
However, we must recognise that empowered local bodies can only facilitate improvements in functioning of public facilities or increasing health awareness, but their actions cannot be a substitute for other critical interventions (improving doctor-patient ratios, overhauling health management system, improving availability of essential medicines, reducing disparities in access to health care etc.) in the health sector. Bihar has the worst doctor to patient ratios and ranks lowest in terms of number of health personnel per capita. Without improving access to healthcare and doctor-patient ratios through systemic reform, meeting the goal of "health for all" would remain elusive in Bihar.
Further Reading
- Bardhan, Pranab, Dilip Mookherjee and MP Torrado (2010), "Impact of political reservations in West Bengal local governments on anti-poverty targeting", Journal of Global Development, 1(1):1-38.
- Chattopadhyay, Raghabendra and Esther Duflo (2004), "Women as Policy Makers: Evidence from a Randomized Policy Experiment in India", Econometrica, 72(5):1409-1443. Available here.
- Bhalotra, Sonia and Irma Clots-Figueras (2014), "Health and the Political Agency of Women", American Economic Journal: Economic Policy, 6:164-97.
- Kumar, Santosh and Nishith Prakash (2017), "Effect of political decentralization and female leadership on institutional births and child mortality in rural Bihar, India", Social Science and Medicine, Vol. 185, pp. 171-178.

Comments will be held for moderation. Your contact information will not be made public.